Loading...
DWIHN, Program Compliance Committee, 6/11/2025
Unknown Speaker
Can you hear me? Okay, I'm
Unknown Speaker
Mr. White, Can you hear us? I
Unknown Speaker
I got you now. Can you hear
Speaker 1
me? Yes, sir, You're all set. All right. Thank You.
Speaker 2
This is Good afternoon. Good afternoon. I am calling to order the program Compliance Committee meeting on today, June 11, Wednesday of 2025,
Unknown Speaker
we will begin with a moment of silence.
Unknown Speaker
Thank you. Lillian, will you do the roll? Call?
Unknown Speaker
Yes. Madam Chair,
Speaker 1
Miss Bullock present. Thank you. Dr Crowder, present. Thank you. Mr. Phillips present. Thank you. Mr. Glenn,
Unknown Speaker
we'll circle back to Mr. Glenn.
Speaker 1
Commissioner Kellogg is excused for today. Dr tag, are you joining the call virtually? Dr tag, are you joining the call virtually?
Unknown Speaker
Are there any board members joining the call virtually?
Unknown Speaker
Mr. White, are you joining us? Virtually? Good
Speaker 1
afternoon. Yes, ma'am, thank you, sir, madam chair, you do have a quorum.
Speaker 2
Thank you, and it's good to hear your voice. Mr. White, we will move on to the approval of the agenda. Is there all
Unknown Speaker
those in favor? Please say aye. Are
Speaker 2
there any nays, abstentions, agenda is approved as presented follow up items from the previous meeting, children's initiatives quarterly report. You
Speaker 3
You think, oh, good afternoon, everyone. Steve. Board members. My name is Cassandra Phipps, and I'm the director of children's initiatives. I am presenting the follow up to the question from the previous board meeting. Provide information on what efforts are in place to reach African American boys between the ages of 10 to 14, to help them before they are in a crisis. This data was shared from our VP of crisis services Grace wolf that that was the most prevalent demographic that was in a crisis care center. So I do have a few you know, areas that I want to share of how we are outreaching to that population. Number one, we're very keen on providing education awareness of behavioral health services and prevention programs in the community. Believe it or not, this is an ongoing effort, because there's still a lot of people, agencies and programs that are unaware of our services. So this is an ongoing initiative that we have throughout the year, and we do have an accessing Community Mental Health presentation that we do throughout the year as well. We do it with the schools. We do it with any agency that reaches out and asks for information. The second area that we are able to reach is with our prevention programs. We have the School Success Initiative, the goal line program, our youth United program, these are positive activities and educational resources to help prevent crisis as well as I will share later in my quarterly report about the youth that are in these programs have a low rate of crisis screenings and hospitalizations. I also want to note that even our providers in the community, they have specialty programs and grant projects. I want to give an example. At the Children's Center, they have their dream builders mentorship group, which offers a parent cafe, a group specifically for African American boys, and a Family Resource Center, and that's just one example. Also our department, we coordinate very much with the Department of Health and Human Services. There's a variety of case consult meetings that we have with them, because a lot of those youth are involved in the child welfare system or they're in foster care, and so we're constantly helping be a resource to that group to connect them to services. Also, we've been looking at the trends of our crisis screenings in Wayne County, and we want to do even a deeper dive in looking at the risk factor trends, the zip codes, where they're coming from, where are they residing. So far, when we looked at the data for fiscal year 24 the most prevalent risk concern was suicidality, so that's suicidal thoughts and suicidal plans. And so we want to go further and looking at, well, where in Wayne County are the these youth coming from? So that way we can better target reaching those, those kids. Also, we do have some new initiatives that we rolled out 
 this year. The first one is the Michigan collaborative, collaborative MC three. This is a project with the University of Michigan. They started a launch a new pilot in the children's hospital emergency room, and so they're providing psychiatric consultation for that emergency room department. The second new initiative that's rolling out is with Southwest counseling solutions. They're also working in the Children's Hospital, and the new program is called the Youth nominated support model. They're specifically targeting African American boys aged 12 to 17 to meet them right when they have an acute risk of suicide. And so those are two new programs that have started this year. And then the last thing I want to say is that we continue to build a qualified workforce. We have a variety of evidence based practices that we are training our professionals on to work with the population. And then also, it helps when you have therapists that looks like the ones that we service. And so doing a survey within our network of how many male therapists do we actually have, I know even our Detroit Wayne Care Clinic outpatient clinic has male therapists, so you know this that goes a long way of being able to be to be relatable for those that are getting treatment and services. And that concludes my follow up.
this year. The first one is the Michigan collaborative, collaborative MC three. This is a project with the University of Michigan. They started a launch a new pilot in the children's hospital emergency room, and so they're providing psychiatric consultation for that emergency room department. The second new initiative that's rolling out is with Southwest counseling solutions. They're also working in the Children's Hospital, and the new program is called the Youth nominated support model. They're specifically targeting African American boys aged 12 to 17 to meet them right when they have an acute risk of suicide. And so those are two new programs that have started this year. And then the last thing I want to say is that we continue to build a qualified workforce. We have a variety of evidence based practices that we are training our professionals on to work with the population. And then also, it helps when you have therapists that looks like the ones that we service. And so doing a survey within our network of how many male therapists do we actually have, I know even our Detroit Wayne Care Clinic outpatient clinic has male therapists, so you know this that goes a long way of being able to be to be relatable for those that are getting treatment and services. And that concludes my follow up.
+3
this year. The first one is the Michigan collaborative, collaborative MC three. This is a project with the University of Michigan. They started a launch a new pilot in the children's hospital emergency room, and so they're providing psychiatric consultation for that emergency room department. The second new initiative that's rolling out is with Southwest counseling solutions. They're also working in the Children's Hospital, and the new program is called the Youth nominated support model. They're specifically targeting African American boys aged 12 to 17 to meet them right when they have an acute risk of suicide. And so those are two new programs that have started this year. And then the last thing I want to say is that we continue to build a qualified workforce. We have a variety of evidence based practices that we are training our professionals on to work with the population. And then also, it helps when you have therapists that looks like the ones that we service. And so doing a survey within our network of how many male therapists do we actually have, I know even our Detroit Wayne Care Clinic outpatient clinic has male therapists, so you know this that goes a long way of being able to be to be relatable for those that are getting treatment and services. And that concludes my follow up. 
Unknown Speaker
Thank you, Miss Phipps, are there any questions?
Speaker 2
One question, yes, you've identified the number one risk for this population of boys, 10 to 14, is suicide. Thought suicide?
Speaker 3
Well, when we looked at the data as a whole of all the children, it was suicidality. And so the age the 10 to 14 are the ones that are going to the crisis care center. So we wanted to look at, well, what is the most prevalent need amongst our in Wayne County for kids that are coming in for crisis and so we can look deeper into that. But that was our preliminary findings.
Unknown Speaker
How will you know you're successful?
Speaker 3
That's a very good question, and that's why we have our Zero Suicide initiative, and that's why, you know, we, when we have our specialty programs, we are tracking outcomes, and that's why you know, even when I share my quarterly report, I'm able to share that for the kids that are in our specialty programs, they're showing a lower risk of crisis screenings and a lower risk of being in a hospital. And so that's showing that they're they're engaged in these positive activities, and they're learning the skills, and that's helping them to be able to manage and control their emotions and offering support to the entire family. So that's another good thing that our services offer is not just for the child, but we're very family centered, and we're making sure that we're really looking towards the whole family being stable, so that's the child and the parent in the community. So that's one of the ways we can show outcomes, and that is, it's working. Yeah. Thank you. Yes. Is
Speaker 4
it trending up each year, or is it, as relates to these this demographic? Is the amount of people that are, you know, going to the crisis center? Is that trending up, or is it flat? Or what's the what's the trend?
Speaker 3
I'll have to defer to our VP of crisis, great school, but I do know this is a, this is a new program that just started this year. So we don't really have, like, previous data on that, because it's a new program. But I will defer to her.
Speaker 5
Hi, Grace will VP of crisis services. The question was whether or not we are seeing more admissions specifically to the children's unit, yeah, to
Unknown Speaker
the demographic of children,
Speaker 5
so specifically to ages 10 through 14. I don't have that data in front of me, I'm happy to pull it and can share that with Lillian. Okay,
Unknown Speaker
thank you. Thank you.
Speaker 2
If they're not, if there aren't any other questions, we will move on. Thank you very much. The outpatient clinics quarterly report.
Unknown Speaker
Good afternoon.
Speaker 6
Good 
 afternoon. Ebony Reynolds, Executive Director of the outpatient clinics, I did include this information in my quarterly report, but I can provide the follow up item now, if that is okay with you, Dr Carter, Madam Chair, okay, so the follow up was provide information on outreach awareness to get more men into outpatient care instead of going to crisis. I have recently recruited male staff. I initially needed a few more male staff on the team, and so we recruited some qualified male clinicians. And part of that is we've begun some planning sessions on some outreach efforts to enroll more men. We've just, I just hired these individuals, so we're just beginning. I'll be able to provide some more information. Some more information on exactly what it is that we intend to do, but we have started. We're looking at a list of locations where we're finding that there are more men participating, that are a part of services. And what we're doing is we're also going to be working with our communications team. We are working together on some partnerships where we can expand our awareness of the outpatient clinic to the community, and we'll be utilizing those men to ensure that they are reaching the target population. And that's it for me, unless there's any questions, are there any questions,
afternoon. Ebony Reynolds, Executive Director of the outpatient clinics, I did include this information in my quarterly report, but I can provide the follow up item now, if that is okay with you, Dr Carter, Madam Chair, okay, so the follow up was provide information on outreach awareness to get more men into outpatient care instead of going to crisis. I have recently recruited male staff. I initially needed a few more male staff on the team, and so we recruited some qualified male clinicians. And part of that is we've begun some planning sessions on some outreach efforts to enroll more men. We've just, I just hired these individuals, so we're just beginning. I'll be able to provide some more information. Some more information on exactly what it is that we intend to do, but we have started. We're looking at a list of locations where we're finding that there are more men participating, that are a part of services. And what we're doing is we're also going to be working with our communications team. We are working together on some partnerships where we can expand our awareness of the outpatient clinic to the community, and we'll be utilizing those men to ensure that they are reaching the target population. And that's it for me, unless there's any questions, are there any questions,
+4
afternoon. Ebony Reynolds, Executive Director of the outpatient clinics, I did include this information in my quarterly report, but I can provide the follow up item now, if that is okay with you, Dr Carter, Madam Chair, okay, so the follow up was provide information on outreach awareness to get more men into outpatient care instead of going to crisis. I have recently recruited male staff. I initially needed a few more male staff on the team, and so we recruited some qualified male clinicians. And part of that is we've begun some planning sessions on some outreach efforts to enroll more men. We've just, I just hired these individuals, so we're just beginning. I'll be able to provide some more information. Some more information on exactly what it is that we intend to do, but we have started. We're looking at a list of locations where we're finding that there are more men participating, that are a part of services. And what we're doing is we're also going to be working with our communications team. We are working together on some partnerships where we can expand our awareness of the outpatient clinic to the community, and we'll be utilizing those men to ensure that they are reaching the target population. And that's it for me, unless there's any questions, are there any questions, 

Speaker 4
is it men overall, or is there, like a demographic or age group within the men that you're seeing an increase in?
Speaker 6
So this was a follow up item, actually, when last month, during our program compliance committee, our Vice President of crisis care services provided her data on the presentations of individuals that she's seen at our crisis stabilization unit, which was kind of a mesh together what Cassandra just did in terms of her response and what I'm presenting here today. There were two requests looking at ages 14 to 17, and then also looking at African American men and men overall. So this is to target men, but if you look at our demographic, which I'll go over with my presentation, 80% of the individuals that we serve right now are African American, and these are where our two current site locations are. So by virtue of the numbers, more more likely we'll be targeting the demographic that I have that we're currently
Speaker 4
a result, though of the fact that you're within a area where it's primarily African American. So whether, whether crisis centers are at,
Unknown Speaker
I'm sorry, do you mind repeating that?
Speaker 4
Is that a result, though of the fact that, because you're in an area where it's primarily African Americans, the natural thought to is that you would see more African Americans than if you were in a much more balanced demographic. I
Speaker 6
think, yes, I mean, you're saying because are you? Basically, you're asking me if, if this because of the fact that we are center in Detroit that we're seeing more African American men. Statistically, yes, that is the data that we have right now. We are seeing more African American men.
Speaker 4
The reason I ask that is because, you know, sometimes we think we may have a crisis, but you know, and I'm not, you know, saying that we don't, but you know, if we're in Detroit, where majority of people are African American. Quite naturally, you you're going to see more African American people the crisis center, because it's because of its proximity. Now, when we open crisis centers down river, whereas, you know, the demographic is a little different. If we're seeing a large number of African Americans going in that crisis center. Then, you know, we have much more of a crisis. We can say now we have a much more of a crisis towards African American men. But you know, just, I just don't want us to get in crisis mode. If you don't have to, I
Speaker 6
understand absolutely we will shift our efforts based on need. So regardless of wherever our site location is. If our data shows that we have a certain population where there is a need to address any particular behavioral health condition, we will be focused on that regardless of wherever our location is. Okay, thank you. Thank you. Why don't
Speaker 2
you just do your RE your quarterly report? Now,
Unknown Speaker
okay, if that's okay with everybody,
Unknown Speaker
is that all right?
Unknown Speaker
Let's see here. Okay, well,
Speaker 6
the  I got, I can start with some good news. Detroit Wayne did receive Joint Commission accreditation. I definitely want to extend a huge thank you to miss Grace Wolf and her director, Raheem Hampton, in addition to our outpatient director Melissa Peters and the team, this was a wonderful effort partnership between both departments, but we did receive full three year accreditation for joint commission. So we're really proud of that. That's outstanding. Congratulations. Thank you that. That is effective April 16, and it will go for the next three years. So at the time of your report, I think we received the information like, literally the next day after I'd already submitted the report. So your report doesn't reflect the actual accreditation, but we did receive it as soon as I right after I sent in your board report. So moving on to our ccbhcs. We submitted some we submitted additional information to MDHHS for our CCBHC application. They requested some additional information on our crisis services and our current catchment area, as well as a new cost report. We've submitted all of that information to the state. We did receive a notification from them on May 30 saying
I got, I can start with some good news. Detroit Wayne did receive Joint Commission accreditation. I definitely want to extend a huge thank you to miss Grace Wolf and her director, Raheem Hampton, in addition to our outpatient director Melissa Peters and the team, this was a wonderful effort partnership between both departments, but we did receive full three year accreditation for joint commission. So we're really proud of that. That's outstanding. Congratulations. Thank you that. That is effective April 16, and it will go for the next three years. So at the time of your report, I think we received the information like, literally the next day after I'd already submitted the report. So your report doesn't reflect the actual accreditation, but we did receive it as soon as I right after I sent in your board report. So moving on to our ccbhcs. We submitted some we submitted additional information to MDHHS for our CCBHC application. They requested some additional information on our crisis services and our current catchment area, as well as a new cost report. We've submitted all of that information to the state. We did receive a notification from them on May 30 saying  that they have submitted all of their all of our information, information to CMS for approval. So we've not heard anything yet, but we are still waiting for notification on that certification. Moving on to our quarter two performance indicators, I did provide some information a couple months ago, but the we are still in the middle of quarter three, so I'm going to go over some more of our quarter more of our quarter two performance indicators. I do have all of the indicators currently that we're required to meet as part of our state contract, and the data points that we have so far had as a clinic. So our first one is indicator two, a that's the request for service within 14 days. I mean, service is delivered within 14 days of a non emergent request for service. For quarter two, we did meet that benchmark. The State benchmark is 57% and I'm having a hard time seeing my own writing here, but we did meet it for quarter two. Indicator three is the individuals who for sorry, oh, beginning services after 14 days of that request. The standard is 83% or above. We met that performance indicator for both children and adults. Indicator four percentage of discharges from a psychiatric inpatient unit who were seen for follow up care within seven days. The standard is 95% or above. We have one inpatient admission for quarter two for an adult, and we did meet that benchmark. Indicator 10 percentage of readmissions. We had the one individual, the standard is 15% and that we did meet the benchmark for that individual, that person did not return to a hospital within 30 days. Just moving on to some of our current enrollment and demographic data, we began providing our
that they have submitted all of their all of our information, information to CMS for approval. So we've not heard anything yet, but we are still waiting for notification on that certification. Moving on to our quarter two performance indicators, I did provide some information a couple months ago, but the we are still in the middle of quarter three, so I'm going to go over some more of our quarter more of our quarter two performance indicators. I do have all of the indicators currently that we're required to meet as part of our state contract, and the data points that we have so far had as a clinic. So our first one is indicator two, a that's the request for service within 14 days. I mean, service is delivered within 14 days of a non emergent request for service. For quarter two, we did meet that benchmark. The State benchmark is 57% and I'm having a hard time seeing my own writing here, but we did meet it for quarter two. Indicator three is the individuals who for sorry, oh, beginning services after 14 days of that request. The standard is 83% or above. We met that performance indicator for both children and adults. Indicator four percentage of discharges from a psychiatric inpatient unit who were seen for follow up care within seven days. The standard is 95% or above. We have one inpatient admission for quarter two for an adult, and we did meet that benchmark. Indicator 10 percentage of readmissions. We had the one individual, the standard is 15% and that we did meet the benchmark for that individual, that person did not return to a hospital within 30 days. Just moving on to some of our current enrollment and demographic data, we began providing our 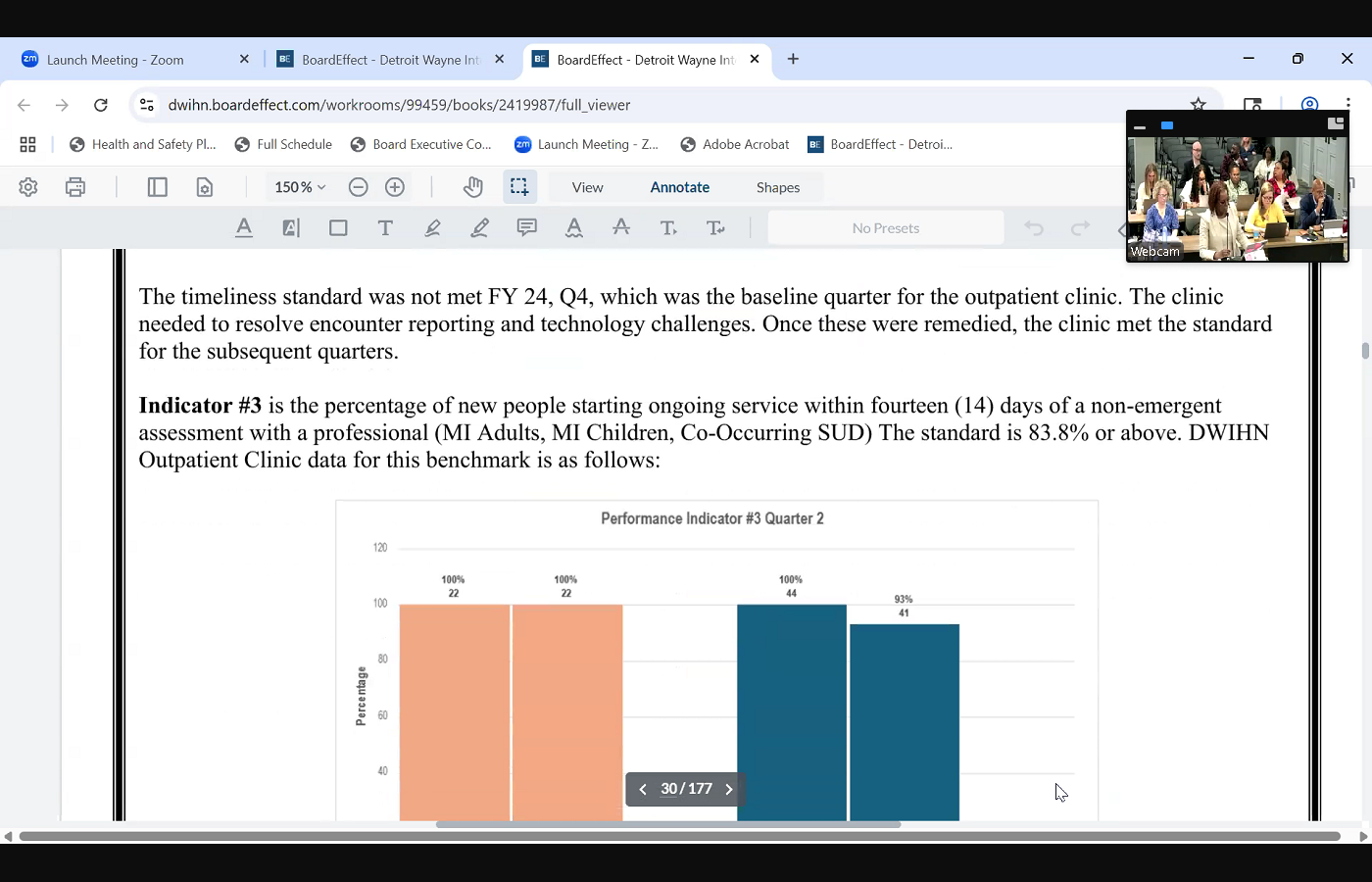
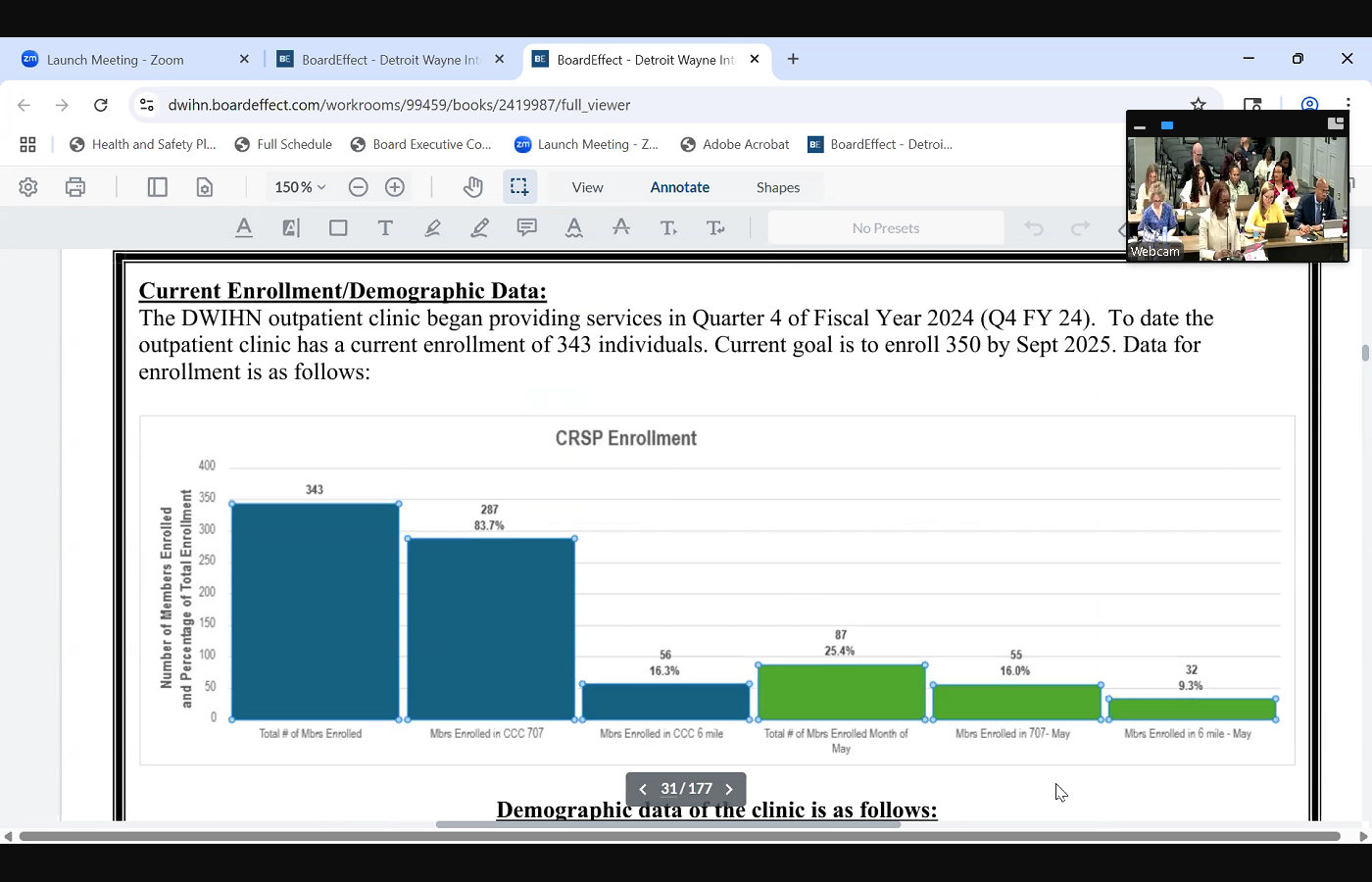 services to for the outpatient clinic quarter four of fiscal year 24 and to date, we have an approximate enrollment of 343 individuals. It is probably increased between last week and now, but we are currently at 343 our goal is to reach 350 individuals by September 25 and I did provide some data on our enrollment. If you can scroll to our crisp enrollment. As you can see, where our members are located, 80, almost 84% of our individuals are currently housed at our seven Oh, not house, receiving services at our 707 site location, and 16% are currently at our six mile location. We are steadily seeing a an increase in enrollment at our six mile location, and we're going to continue to pursue enrolling more individuals there. The next table will show a little bit of demographic data on who we currently serve. Based on our current enrollment, 80% or 80 Yeah, 80% of our individuals are African American, 70% are adults and 30% are children. That is pretty much on target with what we see in terms of overall network as well in their demographic. Our adult members are severe and persistent, persistent mental illness. Our
services to for the outpatient clinic quarter four of fiscal year 24 and to date, we have an approximate enrollment of 343 individuals. It is probably increased between last week and now, but we are currently at 343 our goal is to reach 350 individuals by September 25 and I did provide some data on our enrollment. If you can scroll to our crisp enrollment. As you can see, where our members are located, 80, almost 84% of our individuals are currently housed at our seven Oh, not house, receiving services at our 707 site location, and 16% are currently at our six mile location. We are steadily seeing a an increase in enrollment at our six mile location, and we're going to continue to pursue enrolling more individuals there. The next table will show a little bit of demographic data on who we currently serve. Based on our current enrollment, 80% or 80 Yeah, 80% of our individuals are African American, 70% are adults and 30% are children. That is pretty much on target with what we see in terms of overall network as well in their demographic. Our adult members are severe and persistent, persistent mental illness. Our 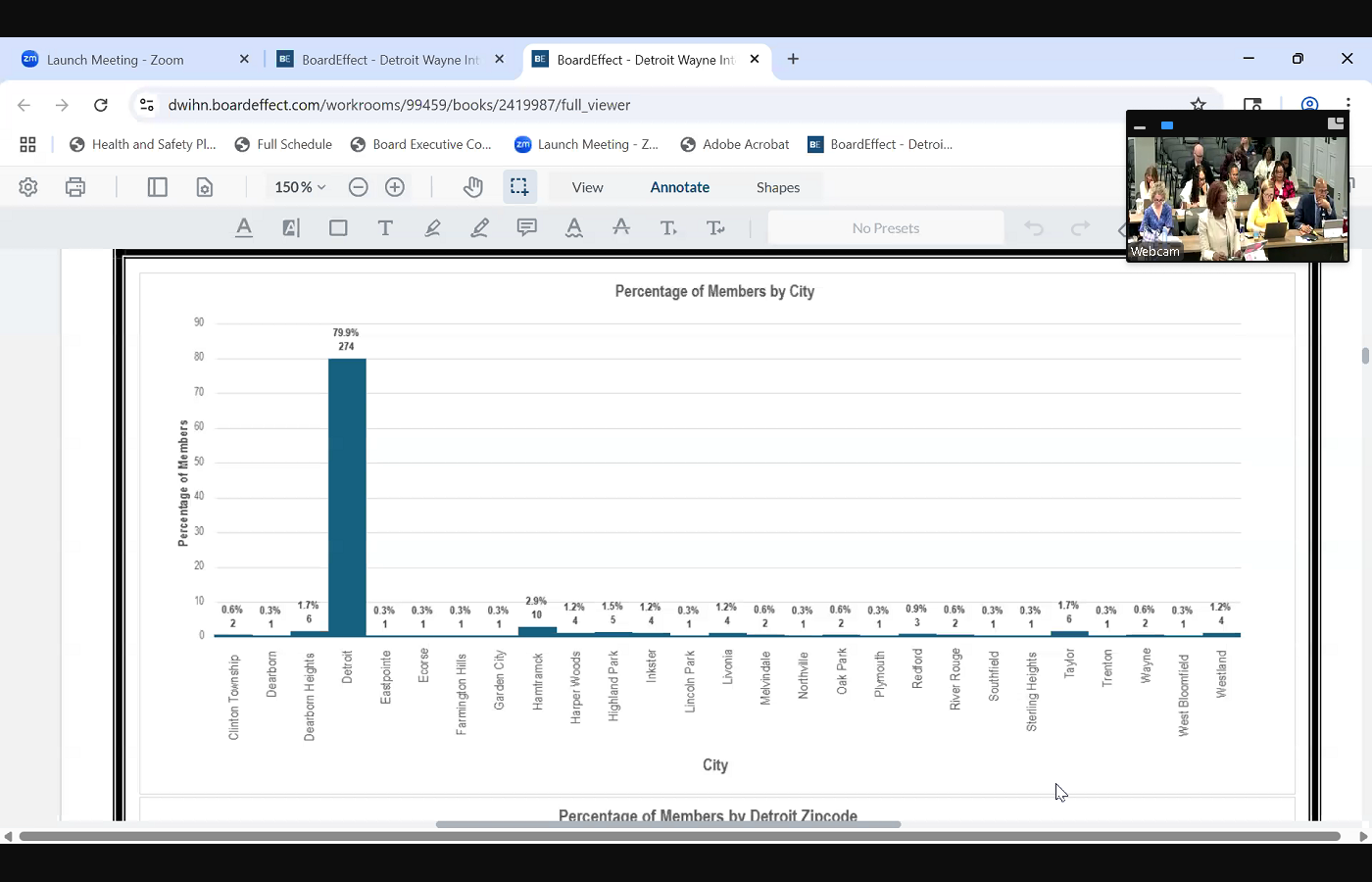
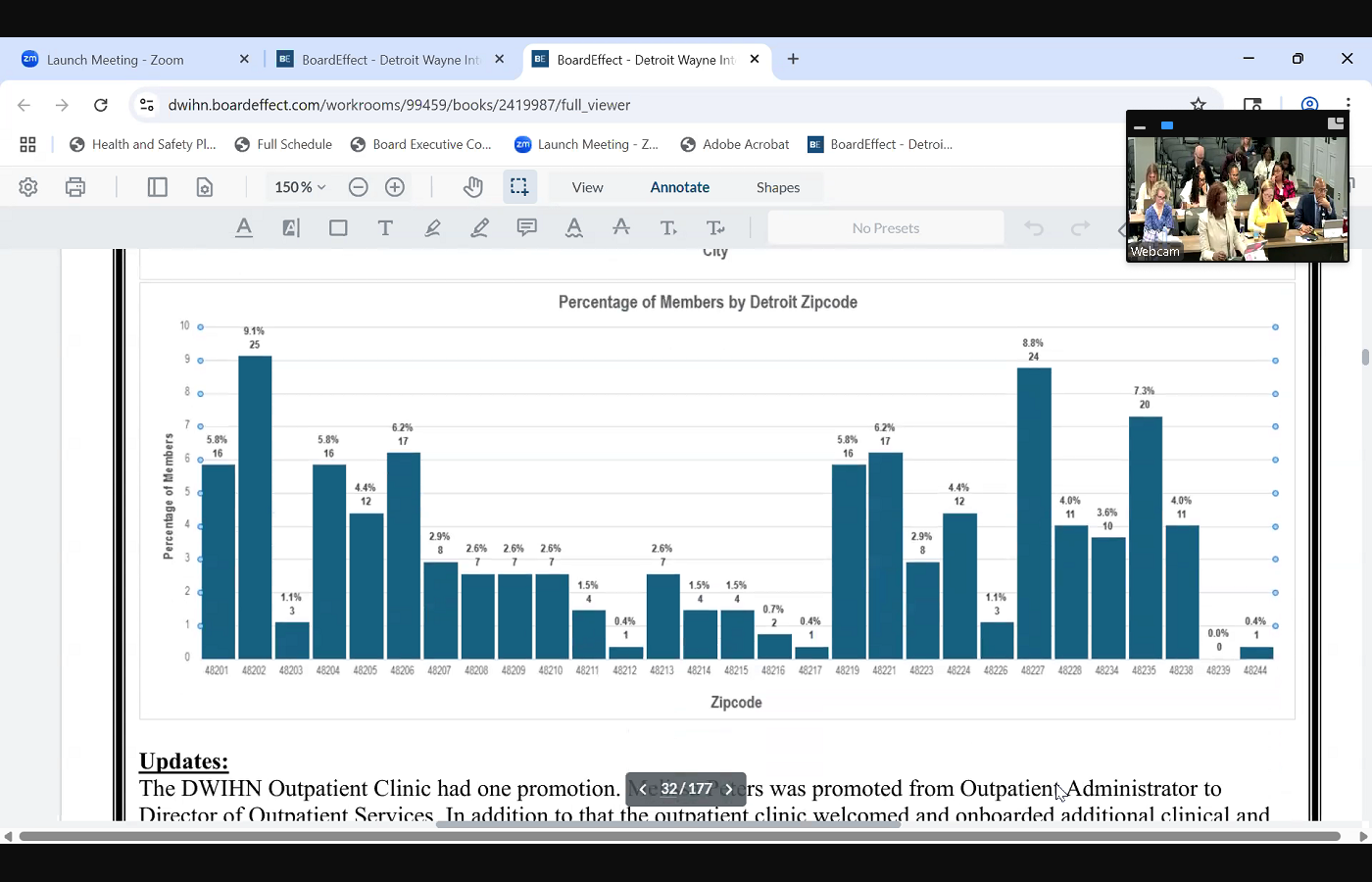 children population, our children with severe and emotional disorders. Moving on to our percentage of members by city, 80% of our enrollees are in the Detroit area. We do have a few individuals that live outside of the Detroit area, but the overwhelming majority, 80% there are Detroit residents. And then lastly, we have our percentage of individuals by zip code for a 202, which is where we are currently, is where most of our individuals are coming from. I believe our next highest is 48227, and 48235, so we are expanding our access across Detroit. Few updates regarding our outpatient clinic. Clinic, we did have one promotion. The outpatient administrator, Melissa Peters, was promoted to director of outpatient services, and we've also onboarded a few additional clinical staff as well to help support the overall operation of the outpatient clinic. Couple things that we're doing well, meeting the benchmarks, we've been working collaborative, collaboratively with our IT department and our program, or PCE, to better capture our performance benchmarks, all of our data. We have a lot of requirements and measurements, so we're building that out. We do have some clinicians that are currently participating in the trauma focused cognitive behavioral therapy cohort. This is a cohort led by the state. This is also one of the evidence based practices required for CCBHC. So we do have clinicians and a supervisor undergoing that cohort that will be very beneficial for us. We also hired and recruited peer support specialists and supported them getting their full peer certified, peer support specialist certification, and we are taking looks as well as some opportunities for improvement. We are looking at some performance improvement plans just to make sure that we're staying on target with what we should be doing, measuring what we should be measuring. We are looking closely at that. And lastly, we do have some partnerships, and as I mentioned earlier, with our communications team, please look to us for some more information coming soon regarding some different branding for the outpatient clinic. We'll be rolling that out shortly, as well as some additional, you know, media opportunities for us to expand information about our clinic. And that concludes my quarterly report.
children population, our children with severe and emotional disorders. Moving on to our percentage of members by city, 80% of our enrollees are in the Detroit area. We do have a few individuals that live outside of the Detroit area, but the overwhelming majority, 80% there are Detroit residents. And then lastly, we have our percentage of individuals by zip code for a 202, which is where we are currently, is where most of our individuals are coming from. I believe our next highest is 48227, and 48235, so we are expanding our access across Detroit. Few updates regarding our outpatient clinic. Clinic, we did have one promotion. The outpatient administrator, Melissa Peters, was promoted to director of outpatient services, and we've also onboarded a few additional clinical staff as well to help support the overall operation of the outpatient clinic. Couple things that we're doing well, meeting the benchmarks, we've been working collaborative, collaboratively with our IT department and our program, or PCE, to better capture our performance benchmarks, all of our data. We have a lot of requirements and measurements, so we're building that out. We do have some clinicians that are currently participating in the trauma focused cognitive behavioral therapy cohort. This is a cohort led by the state. This is also one of the evidence based practices required for CCBHC. So we do have clinicians and a supervisor undergoing that cohort that will be very beneficial for us. We also hired and recruited peer support specialists and supported them getting their full peer certified, peer support specialist certification, and we are taking looks as well as some opportunities for improvement. We are looking at some performance improvement plans just to make sure that we're staying on target with what we should be doing, measuring what we should be measuring. We are looking closely at that. And lastly, we do have some partnerships, and as I mentioned earlier, with our communications team, please look to us for some more information coming soon regarding some different branding for the outpatient clinic. We'll be rolling that out shortly, as well as some additional, you know, media opportunities for us to expand information about our clinic. And that concludes my quarterly report.
+1
I got, I can start with some good news. Detroit Wayne did receive Joint Commission accreditation. I definitely want to extend a huge thank you to miss Grace Wolf and her director, Raheem Hampton, in addition to our outpatient director Melissa Peters and the team, this was a wonderful effort partnership between both departments, but we did receive full three year accreditation for joint commission. So we're really proud of that. That's outstanding. Congratulations. Thank you that. That is effective April 16, and it will go for the next three years. So at the time of your report, I think we received the information like, literally the next day after I'd already submitted the report. So your report doesn't reflect the actual accreditation, but we did receive it as soon as I right after I sent in your board report. So moving on to our ccbhcs. We submitted some we submitted additional information to MDHHS for our CCBHC application. They requested some additional information on our crisis services and our current catchment area, as well as a new cost report. We've submitted all of that information to the state. We did receive a notification from them on May 30 saying +1
that they have submitted all of their all of our information, information to CMS for approval. So we've not heard anything yet, but we are still waiting for notification on that certification. Moving on to our quarter two performance indicators, I did provide some information a couple months ago, but the we are still in the middle of quarter three, so I'm going to go over some more of our quarter more of our quarter two performance indicators. I do have all of the indicators currently that we're required to meet as part of our state contract, and the data points that we have so far had as a clinic. So our first one is indicator two, a that's the request for service within 14 days. I mean, service is delivered within 14 days of a non emergent request for service. For quarter two, we did meet that benchmark. The State benchmark is 57% and I'm having a hard time seeing my own writing here, but we did meet it for quarter two. Indicator three is the individuals who for sorry, oh, beginning services after 14 days of that request. The standard is 83% or above. We met that performance indicator for both children and adults. Indicator four percentage of discharges from a psychiatric inpatient unit who were seen for follow up care within seven days. The standard is 95% or above. We have one inpatient admission for quarter two for an adult, and we did meet that benchmark. Indicator 10 percentage of readmissions. We had the one individual, the standard is 15% and that we did meet the benchmark for that individual, that person did not return to a hospital within 30 days. Just moving on to some of our current enrollment and demographic data, we began providing our +3
services to for the outpatient clinic quarter four of fiscal year 24 and to date, we have an approximate enrollment of 343 individuals. It is probably increased between last week and now, but we are currently at 343 our goal is to reach 350 individuals by September 25 and I did provide some data on our enrollment. If you can scroll to our crisp enrollment. As you can see, where our members are located, 80, almost 84% of our individuals are currently housed at our seven Oh, not house, receiving services at our 707 site location, and 16% are currently at our six mile location. We are steadily seeing a an increase in enrollment at our six mile location, and we're going to continue to pursue enrolling more individuals there. The next table will show a little bit of demographic data on who we currently serve. Based on our current enrollment, 80% or 80 Yeah, 80% of our individuals are African American, 70% are adults and 30% are children. That is pretty much on target with what we see in terms of overall network as well in their demographic. Our adult members are severe and persistent, persistent mental illness. Our 
+3
children population, our children with severe and emotional disorders. Moving on to our percentage of members by city, 80% of our enrollees are in the Detroit area. We do have a few individuals that live outside of the Detroit area, but the overwhelming majority, 80% there are Detroit residents. And then lastly, we have our percentage of individuals by zip code for a 202, which is where we are currently, is where most of our individuals are coming from. I believe our next highest is 48227, and 48235, so we are expanding our access across Detroit. Few updates regarding our outpatient clinic. Clinic, we did have one promotion. The outpatient administrator, Melissa Peters, was promoted to director of outpatient services, and we've also onboarded a few additional clinical staff as well to help support the overall operation of the outpatient clinic. Couple things that we're doing well, meeting the benchmarks, we've been working collaborative, collaboratively with our IT department and our program, or PCE, to better capture our performance benchmarks, all of our data. We have a lot of requirements and measurements, so we're building that out. We do have some clinicians that are currently participating in the trauma focused cognitive behavioral therapy cohort. This is a cohort led by the state. This is also one of the evidence based practices required for CCBHC. So we do have clinicians and a supervisor undergoing that cohort that will be very beneficial for us. We also hired and recruited peer support specialists and supported them getting their full peer certified, peer support specialist certification, and we are taking looks as well as some opportunities for improvement. We are looking at some performance improvement plans just to make sure that we're staying on target with what we should be doing, measuring what we should be measuring. We are looking closely at that. And lastly, we do have some partnerships, and as I mentioned earlier, with our communications team, please look to us for some more information coming soon regarding some different branding for the outpatient clinic. We'll be rolling that out shortly, as well as some additional, you know, media opportunities for us to expand information about our clinic. And that concludes my quarterly report. 
Unknown Speaker
Thank you. Are there any questions?
Unknown Speaker
Yes, please. Hi.
Speaker 7
I'm curious. I noticed in your report, you said you're developing a dashboard in power. Bi, do you have a timeline for that? I'd love to see how that's going. When it will it be soon? Yep. So
Speaker 6
we we have a couple pages that are already there that we're working on right now. I am going to work with the IT department to actually get a timeline. What's beneficial about having some really good colleagues is that one of them listen, heard what we needed, and just kind of started moving forward with putting things into place in partnership with us. So I do appreciate Keith and his team on doing that. I can get you a timeline of when it's actually complete. Though, our first step was actually So through our PCE system, they are able to collect some data points for us, but with the Power BI dashboard, it will help us have a little bit more of a drill down where we can actually look at different measures in terms of engagement by clinician who's having more no shows, cancelations, reschedules, things of that nature. So once it's complete, I have no problem providing a timeline, and that's being built internally. That is being built internally. Yes, thank you.
Unknown Speaker
Any other questions? Mr. Phillips, no.
Unknown Speaker
Great. Thank you. Thank you.
Speaker 2
Now we will go back to follow up items from the previous meeting. The next is the impact of grants not continuing past the first quarter.
Speaker 8
That 
 would be me. Thank you. Thank you, Madam Chair and board members. Melissa moody, VP of Clinical Operations, to give an update, this was sent forward from the finance committee to talk a little bit more about the programmatic side of the ARPA grant COVID funding that was discontinued March 31 of this year. So we had six months in funding available, and then, obviously, we know that was discontinued as of the end of March, we had a total of over $1.7 million in ARPA grant funding that funded 11 different initiatives during that time, most of them, eight of those 11 initiatives were related to substance use services, and I can tell you, for the first six months, we used approximately 46% of those funds. It is a lower amount, and I'll explain that in a minute as to why that's the case. But I just want to talk a little bit about the Sud funding where it stands and those programs. So of those eight programs, we are able to continue a good majority, almost all of these programs. We have three of the programs, the Quick Response Teams, recovery, housing, recovery supports, that all can be fee for service build codes, so that's something that the providers can continue to do and get reimbursed for those services. We also have social activities. There's evidence based practice and prevention and Student Assistance programing. And there is funds through different various sources for that as well, through the Sora grants block grant and PA, two funds. So these are things that we can continue forward. I also want to say, when you look just at those services that directly impact the members, it's actually not 46% it's more than 70% of those funds have been used. What you're going to see the differences, and that's part two of this question that came actually, Part D is about the Mental Health Act fund, that is the majority of the funds that have been left. So of the $538,000
would be me. Thank you. Thank you, Madam Chair and board members. Melissa moody, VP of Clinical Operations, to give an update, this was sent forward from the finance committee to talk a little bit more about the programmatic side of the ARPA grant COVID funding that was discontinued March 31 of this year. So we had six months in funding available, and then, obviously, we know that was discontinued as of the end of March, we had a total of over $1.7 million in ARPA grant funding that funded 11 different initiatives during that time, most of them, eight of those 11 initiatives were related to substance use services, and I can tell you, for the first six months, we used approximately 46% of those funds. It is a lower amount, and I'll explain that in a minute as to why that's the case. But I just want to talk a little bit about the Sud funding where it stands and those programs. So of those eight programs, we are able to continue a good majority, almost all of these programs. We have three of the programs, the Quick Response Teams, recovery, housing, recovery supports, that all can be fee for service build codes, so that's something that the providers can continue to do and get reimbursed for those services. We also have social activities. There's evidence based practice and prevention and Student Assistance programing. And there is funds through different various sources for that as well, through the Sora grants block grant and PA, two funds. So these are things that we can continue forward. I also want to say, when you look just at those services that directly impact the members, it's actually not 46% it's more than 70% of those funds have been used. What you're going to see the differences, and that's part two of this question that came actually, Part D is about the Mental Health Act fund, that is the majority of the funds that have been left. So of the $538,000
+4
would be me. Thank you. Thank you, Madam Chair and board members. Melissa moody, VP of Clinical Operations, to give an update, this was sent forward from the finance committee to talk a little bit more about the programmatic side of the ARPA grant COVID funding that was discontinued March 31 of this year. So we had six months in funding available, and then, obviously, we know that was discontinued as of the end of March, we had a total of over $1.7 million in ARPA grant funding that funded 11 different initiatives during that time, most of them, eight of those 11 initiatives were related to substance use services, and I can tell you, for the first six months, we used approximately 46% of those funds. It is a lower amount, and I'll explain that in a minute as to why that's the case. But I just want to talk a little bit about the Sud funding where it stands and those programs. So of those eight programs, we are able to continue a good majority, almost all of these programs. We have three of the programs, the Quick Response Teams, recovery, housing, recovery supports, that all can be fee for service build codes, so that's something that the providers can continue to do and get reimbursed for those services. We also have social activities. There's evidence based practice and prevention and Student Assistance programing. And there is funds through different various sources for that as well, through the Sora grants block grant and PA, two funds. So these are things that we can continue forward. I also want to say, when you look just at those services that directly impact the members, it's actually not 46% it's more than 70% of those funds have been used. What you're going to see the differences, and that's part two of this question that came actually, Part D is about the Mental Health Act fund, that is the majority of the funds that have been left. So of the $538,000 

Unknown Speaker
that we received that program, we had 429,000
Speaker 8
left. What that program is specifically is for our sort of community treatment team providers. It did not go directly to members or services. It was directly put in place as an incentive program for hiring. Act services are a very intensive community based service. It's traditionally hard to find workers for that program. So that was an incentive program to for the providers to be able to offer hiring incentives, bonuses, retention, training and things like that. So we did have four of the seven of the ACT team. Providers did use expenses towards that we had three providers that did not submit any expenses on that particular line item. And then we also had three other initiatives that were related to staff incentives, training supplies and materials for our CIT and Mental Health First Aid and some allocation for Sud administrative expenses. Thank
Unknown Speaker
you. Other questions, yeah, was the the
Speaker 4
monies that weren't spent? Where I was confused, are those Arbor dollars as well?
Speaker 8
These are all ARPA dollars, yeah. And so
Speaker 4
generally, Arbor dollars have a timeline associated with them. Have we passed the timeline? Yes,
Speaker 8
these funds were discontinued March 31 Okay, so that's where the question was asked about, you know, the programing that was attached to these are we able to continue those programming so we've looked in and identified alternative resources for that. Okay?
Unknown Speaker
Any other questions in this book?
Unknown Speaker
Thank you. Thank you.
Unknown Speaker
Thank you.
Unknown Speaker
Approval of the minutes from May of 2025,
Unknown Speaker
Move for approval. Or all
Unknown Speaker
those in favor, please say aye,
Speaker 2
any nays or abstentions minutes approved from May
Speaker 1
Madam Chair, yes, there was one additional item under follow up, item
Speaker 2
D, provide information on the Mental Health Act fund.
Speaker 8
Yeah, I still got that. Thank you. Yeah,
Unknown Speaker
it was included, but thank you. Lillian,
Speaker 2
the  chief medical officer, and the corporate compliance reports have been deferred until next month's meeting, so we will go on to the quarterly reports, beginning with autism spectrum disorder. You Cassandra,
chief medical officer, and the corporate compliance reports have been deferred until next month's meeting, so we will go on to the quarterly reports, beginning with autism spectrum disorder. You Cassandra,
+1
chief medical officer, and the corporate compliance reports have been deferred until next month's meeting, so we will go on to the quarterly reports, beginning with autism spectrum disorder. You Cassandra, Speaker 3
good 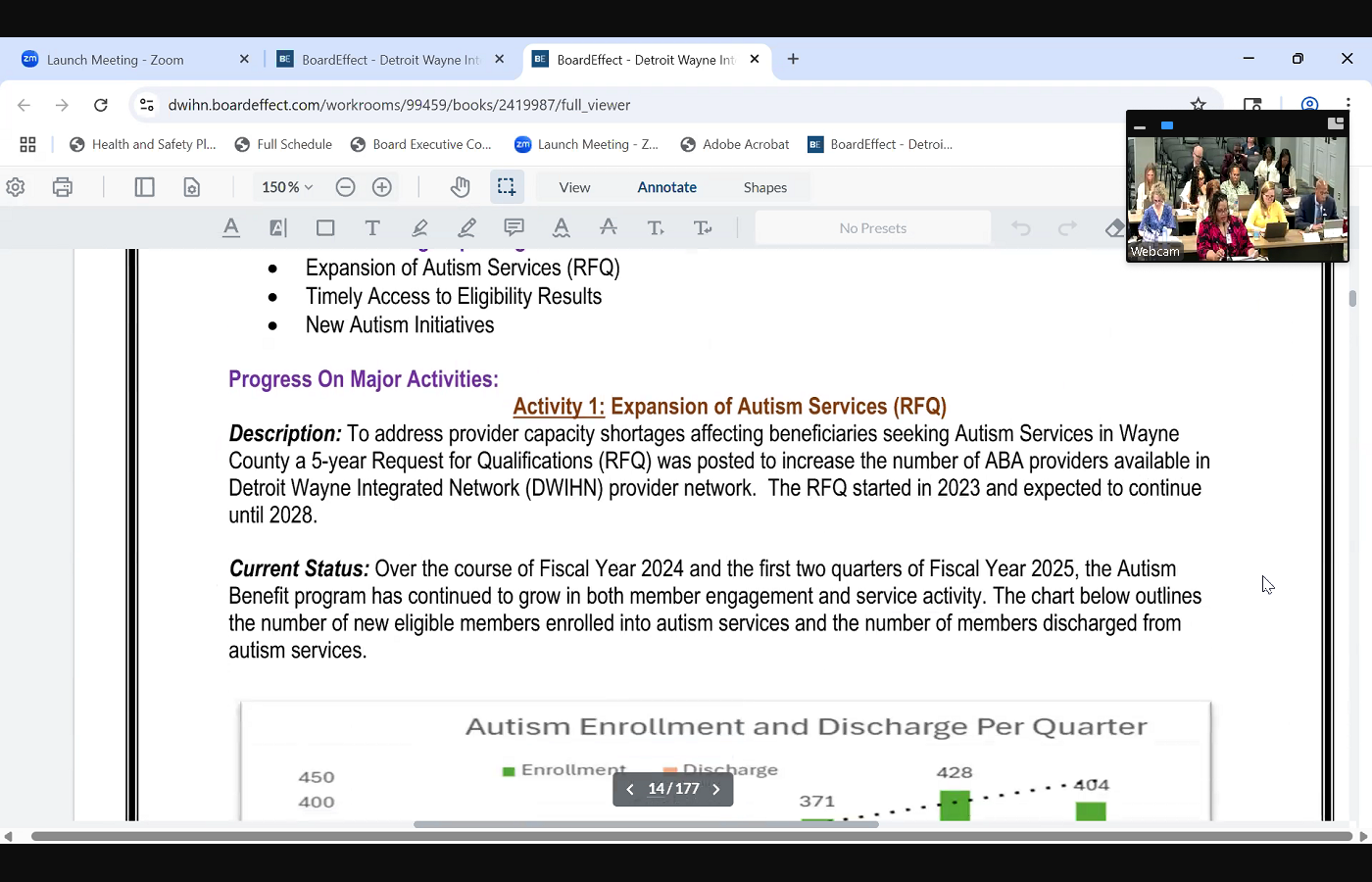
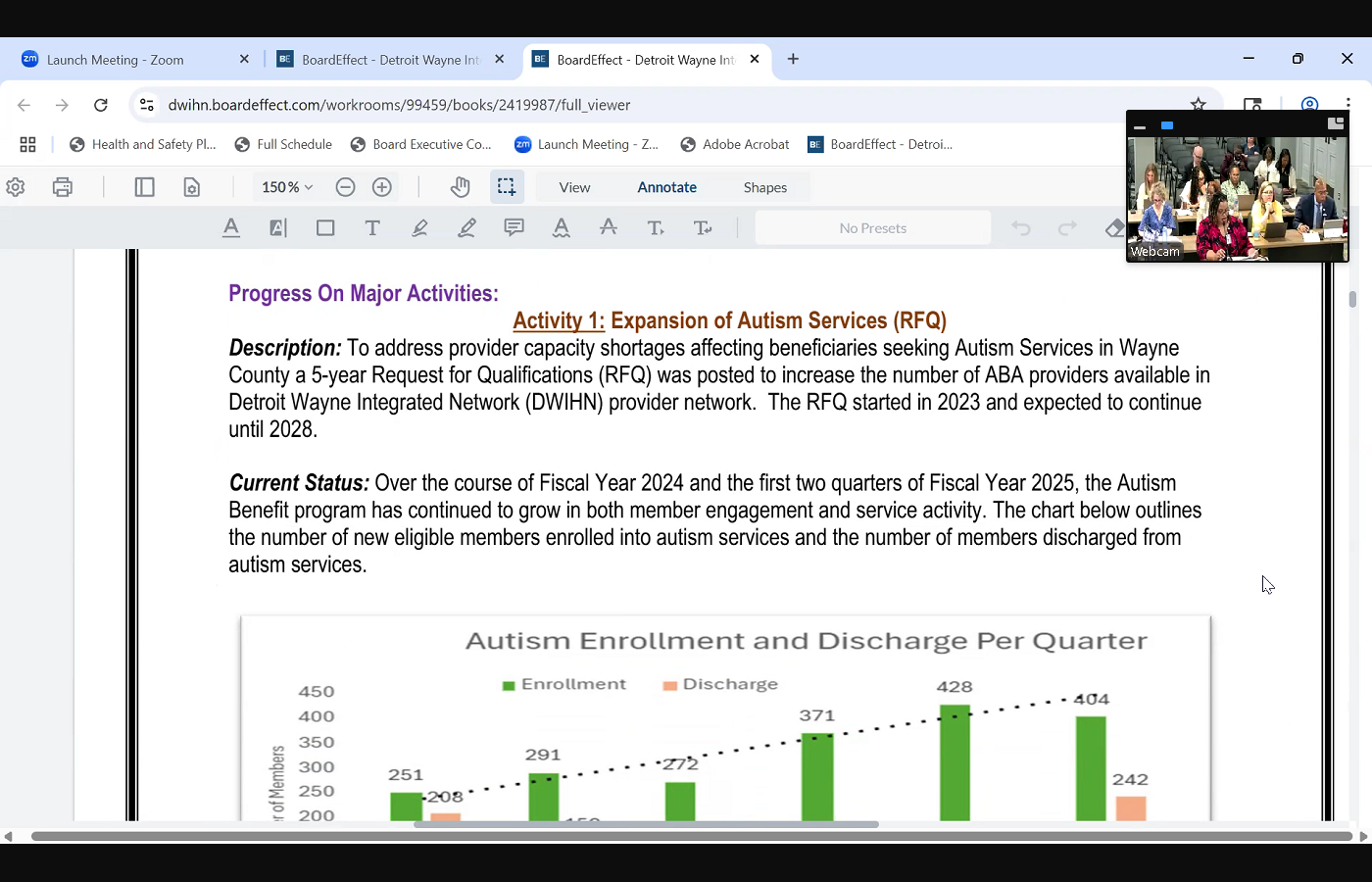 afternoon again. Cassandra Phipps, Director of children's initiatives, and I will be presenting on the autism quarter two report. The three areas I'm going to focus on the expansion of autism services, timely access for services and new initiatives. So when it comes to expansion of autism services, we do have an active request for qualifications, otherwise known as RFQ. This is a five year RFQ, and we have seen an increase of enrollment with youth that are participating in autism services. And so as the chart indicates, for quarter two, there were 404 new children in autism services and 242 discharges. This is an upward trend, trend over the last fiscal year, also when it comes to new providers, we originally started with 15 ABA providers. We're now we had 10 new providers. Eight are currently pending going through the credentialing process, and so we continue to assess the need and move forward accordingly, with making sure that children are able to receive ABA services adequately. When it comes to timely access to services, one of the key areas of improvement that we've been working on is reducing any delays. Once an evaluation has been completed, we want to
afternoon again. Cassandra Phipps, Director of children's initiatives, and I will be presenting on the autism quarter two report. The three areas I'm going to focus on the expansion of autism services, timely access for services and new initiatives. So when it comes to expansion of autism services, we do have an active request for qualifications, otherwise known as RFQ. This is a five year RFQ, and we have seen an increase of enrollment with youth that are participating in autism services. And so as the chart indicates, for quarter two, there were 404 new children in autism services and 242 discharges. This is an upward trend, trend over the last fiscal year, also when it comes to new providers, we originally started with 15 ABA providers. We're now we had 10 new providers. Eight are currently pending going through the credentialing process, and so we continue to assess the need and move forward accordingly, with making sure that children are able to receive ABA services adequately. When it comes to timely access to services, one of the key areas of improvement that we've been working on is reducing any delays. Once an evaluation has been completed, we want to 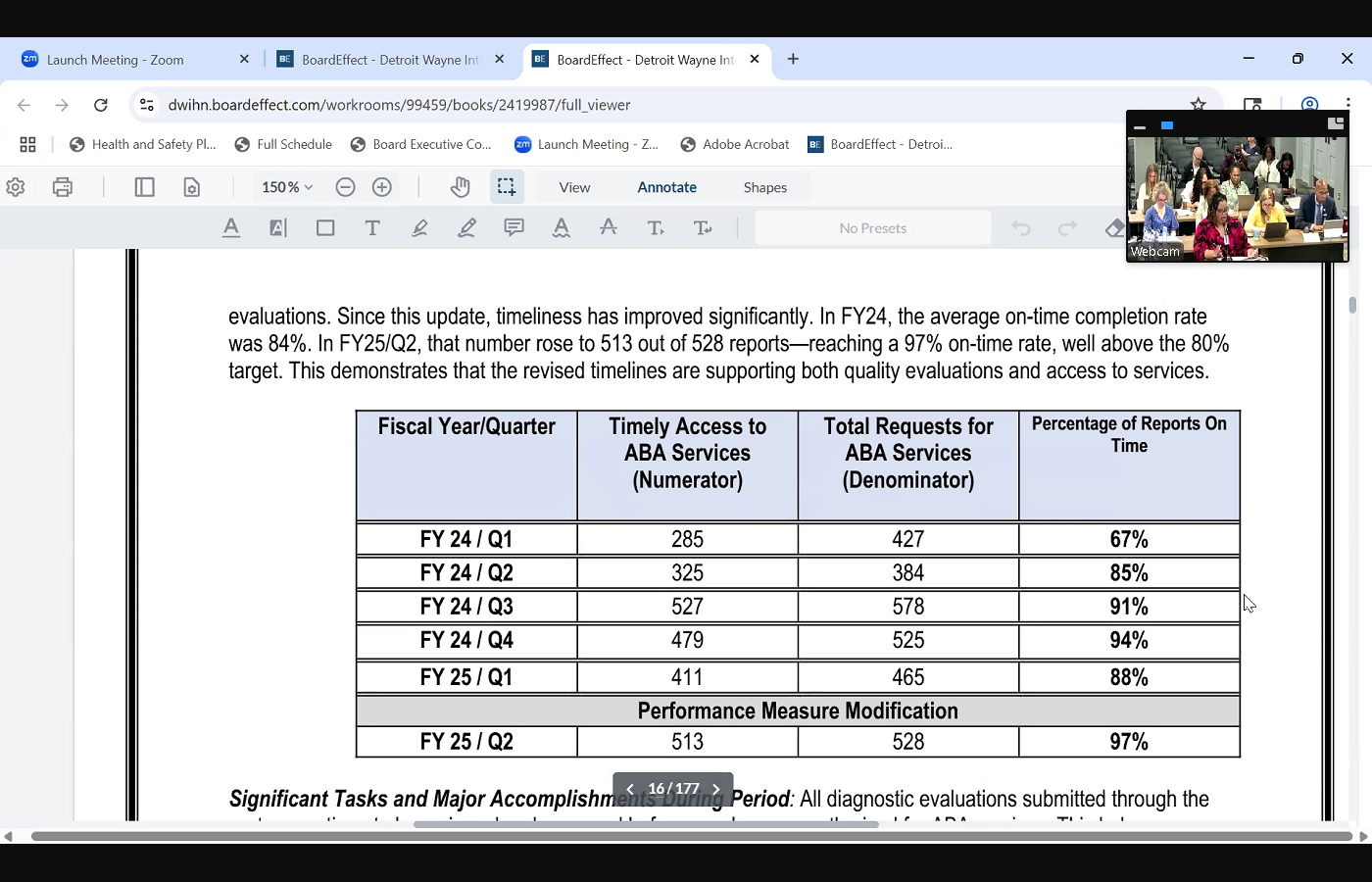
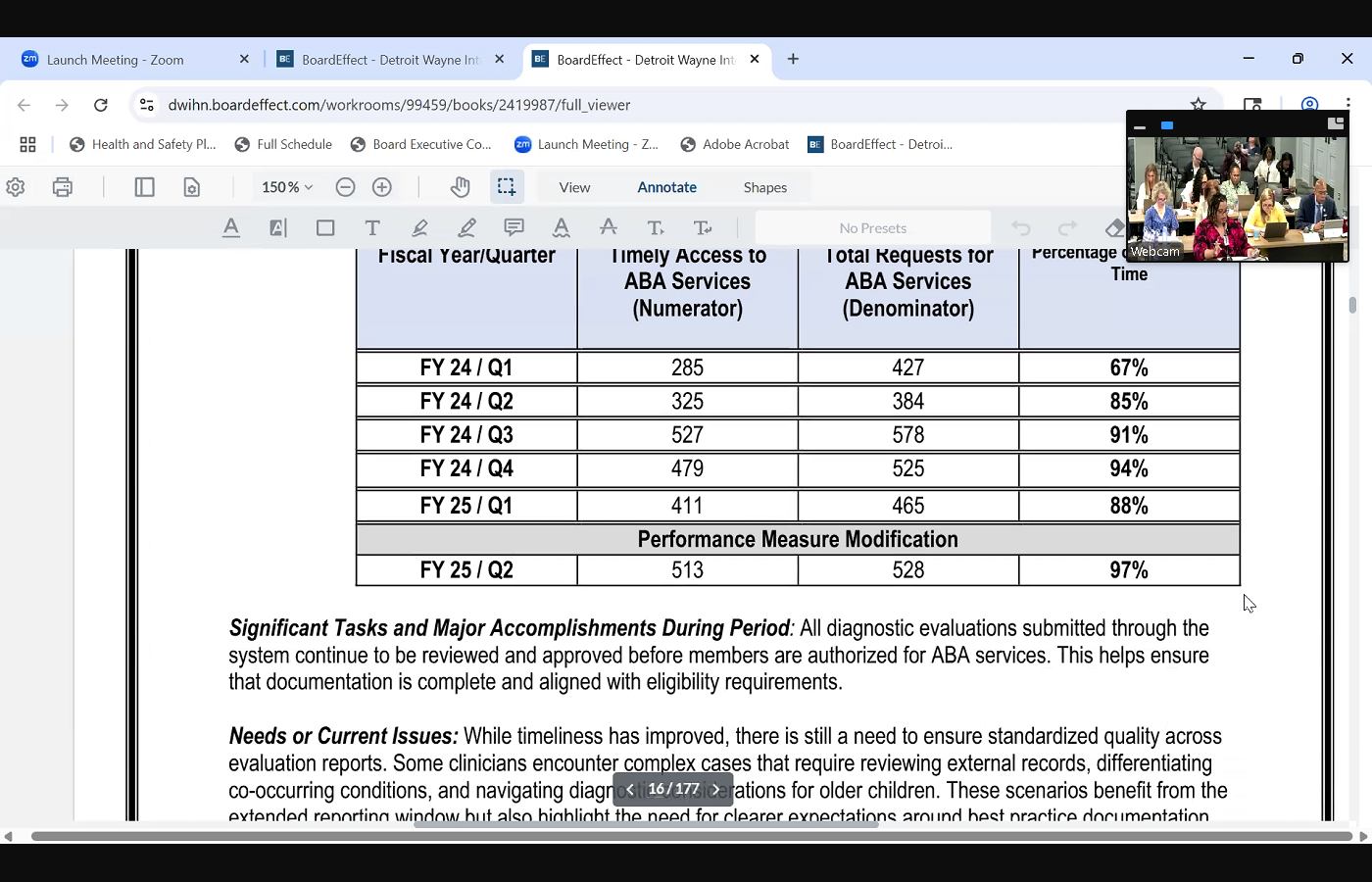 make sure that children are able to start the services and so for those children that resulted in a non autism diagnosis, they have seven days to complete their evaluation. And for those that do have an autism diagnosis, they have 15 business days. And so we are seeing that we are doing well in this area, and we've improved from last fiscal year. So for quarter two, there was we were at 97% of completing evaluations on time, which is above the 80% goal areas that we continue to work on is in addition to the evaluations being completed, the autism evaluators are also supposed to provide feedback sessions with the families, and so that's something that we're also streamlining and following up on to ensure that that's happening adequately, because the state of Michigan is going to be looking at that when it comes to new initiatives for this year, we've really worked on coordinating With our providers, especially onboarding our new providers and streamlining our enrollment and discharge processes as well. And so we piloted the new ABA enrollment and discharge and transfer form, and then also the provider availability form as well. And I just want to conclude with a few final updates. We've hosted a meet and greet and a provider training to strengthen our relationships with our ABA providers. We've onboarded all of the new ABA providers and offered them an image when, which is our electronic health record training. And April was Autism Awareness Month, and so we did a lot of promotion for the month of May as well. And we have new one, new staff person. Her name is Jessica Riley, and she's the new autism specialist benefits person on the autism team. And that concludes my the autism report. Thank
make sure that children are able to start the services and so for those children that resulted in a non autism diagnosis, they have seven days to complete their evaluation. And for those that do have an autism diagnosis, they have 15 business days. And so we are seeing that we are doing well in this area, and we've improved from last fiscal year. So for quarter two, there was we were at 97% of completing evaluations on time, which is above the 80% goal areas that we continue to work on is in addition to the evaluations being completed, the autism evaluators are also supposed to provide feedback sessions with the families, and so that's something that we're also streamlining and following up on to ensure that that's happening adequately, because the state of Michigan is going to be looking at that when it comes to new initiatives for this year, we've really worked on coordinating With our providers, especially onboarding our new providers and streamlining our enrollment and discharge processes as well. And so we piloted the new ABA enrollment and discharge and transfer form, and then also the provider availability form as well. And I just want to conclude with a few final updates. We've hosted a meet and greet and a provider training to strengthen our relationships with our ABA providers. We've onboarded all of the new ABA providers and offered them an image when, which is our electronic health record training. And April was Autism Awareness Month, and so we did a lot of promotion for the month of May as well. And we have new one, new staff person. Her name is Jessica Riley, and she's the new autism specialist benefits person on the autism team. And that concludes my the autism report. Thank
+3
afternoon again. Cassandra Phipps, Director of children's initiatives, and I will be presenting on the autism quarter two report. The three areas I'm going to focus on the expansion of autism services, timely access for services and new initiatives. So when it comes to expansion of autism services, we do have an active request for qualifications, otherwise known as RFQ. This is a five year RFQ, and we have seen an increase of enrollment with youth that are participating in autism services. And so as the chart indicates, for quarter two, there were 404 new children in autism services and 242 discharges. This is an upward trend, trend over the last fiscal year, also when it comes to new providers, we originally started with 15 ABA providers. We're now we had 10 new providers. Eight are currently pending going through the credentialing process, and so we continue to assess the need and move forward accordingly, with making sure that children are able to receive ABA services adequately. When it comes to timely access to services, one of the key areas of improvement that we've been working on is reducing any delays. Once an evaluation has been completed, we want to 
+3
make sure that children are able to start the services and so for those children that resulted in a non autism diagnosis, they have seven days to complete their evaluation. And for those that do have an autism diagnosis, they have 15 business days. And so we are seeing that we are doing well in this area, and we've improved from last fiscal year. So for quarter two, there was we were at 97% of completing evaluations on time, which is above the 80% goal areas that we continue to work on is in addition to the evaluations being completed, the autism evaluators are also supposed to provide feedback sessions with the families, and so that's something that we're also streamlining and following up on to ensure that that's happening adequately, because the state of Michigan is going to be looking at that when it comes to new initiatives for this year, we've really worked on coordinating With our providers, especially onboarding our new providers and streamlining our enrollment and discharge processes as well. And so we piloted the new ABA enrollment and discharge and transfer form, and then also the provider availability form as well. And I just want to conclude with a few final updates. We've hosted a meet and greet and a provider training to strengthen our relationships with our ABA providers. We've onboarded all of the new ABA providers and offered them an image when, which is our electronic health record training. And April was Autism Awareness Month, and so we did a lot of promotion for the month of May as well. And we have new one, new staff person. Her name is Jessica Riley, and she's the new autism specialist benefits person on the autism team. And that concludes my the autism report. Thank 
Unknown Speaker
you. Are there any questions?
Speaker 2
No. Questions. You can move on. I know you have one more report for us
Speaker 3
all 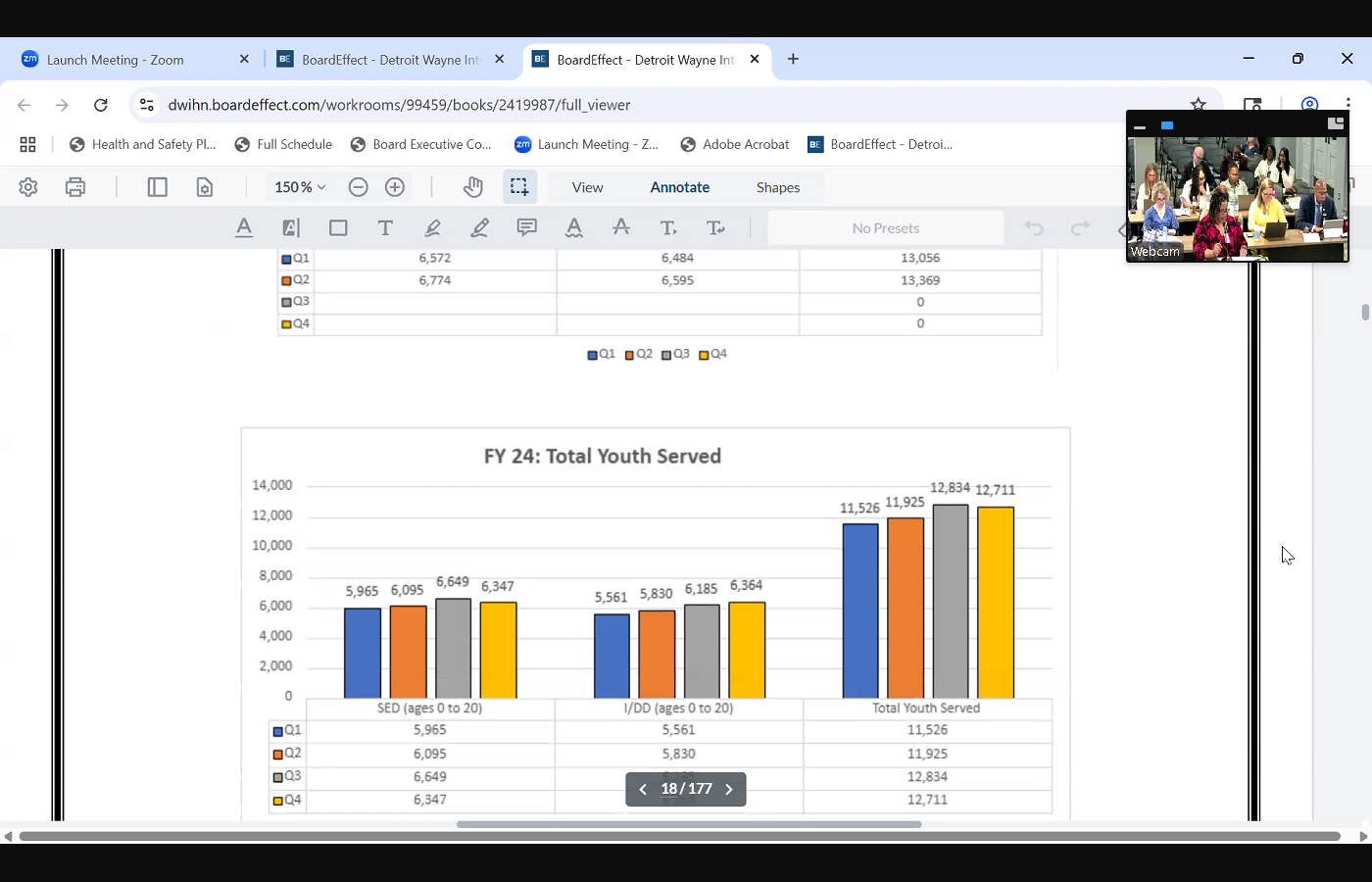
 right. So for the quarter two, children's initiatives report, I want to start by just giving an overview of our census here. So for quarter two, we served an average of 13,369 unduplicated children, youth and families in Wayne County. This is for ages zero to their 21st birthday. Also includes those with serious emotional disturbances and intellectual developmental disabilities. This total is slightly higher than the first quarter, and it's also higher than quarter two of last year. And so as of quarter two, the total number is 26,425 so we continue to grow. The three areas that I'm going to focus on today is access to Children Services, the School Success Initiative Program and a new program, which is the pediatric integrated health program. When it comes to access to services, the state of Michigan implemented a new goal for fiscal year 25 that we have to be at 57% for whenever children have a screening completed, that that intake assessment happens within 14 days. This has been an area that we have struggled in over the last year or so, and so I am happy to inform that for quarter two, we were at 62% and which is higher than the 57% goal. There's a lot of efforts that have went into this. Shout out to our quality department and our IT department that helped us, because what we realized was that there were children specialty programs where the children providers were completing screenings, and that was not being factored into our reporting, and so we worked on rolling out a new screening code and including that into the report. And so we were able to reach the goal. The second program I want to highlight is our School Success Initiative Program. This is where we have
right. So for the quarter two, children's initiatives report, I want to start by just giving an overview of our census here. So for quarter two, we served an average of 13,369 unduplicated children, youth and families in Wayne County. This is for ages zero to their 21st birthday. Also includes those with serious emotional disturbances and intellectual developmental disabilities. This total is slightly higher than the first quarter, and it's also higher than quarter two of last year. And so as of quarter two, the total number is 26,425 so we continue to grow. The three areas that I'm going to focus on today is access to Children Services, the School Success Initiative Program and a new program, which is the pediatric integrated health program. When it comes to access to services, the state of Michigan implemented a new goal for fiscal year 25 that we have to be at 57% for whenever children have a screening completed, that that intake assessment happens within 14 days. This has been an area that we have struggled in over the last year or so, and so I am happy to inform that for quarter two, we were at 62% and which is higher than the 57% goal. There's a lot of efforts that have went into this. Shout out to our quality department and our IT department that helped us, because what we realized was that there were children specialty programs where the children providers were completing screenings, and that was not being factored into our reporting, and so we worked on rolling out a new screening code and including that into the report. And so we were able to reach the goal. The second program I want to highlight is our School Success Initiative Program. This is where we have 
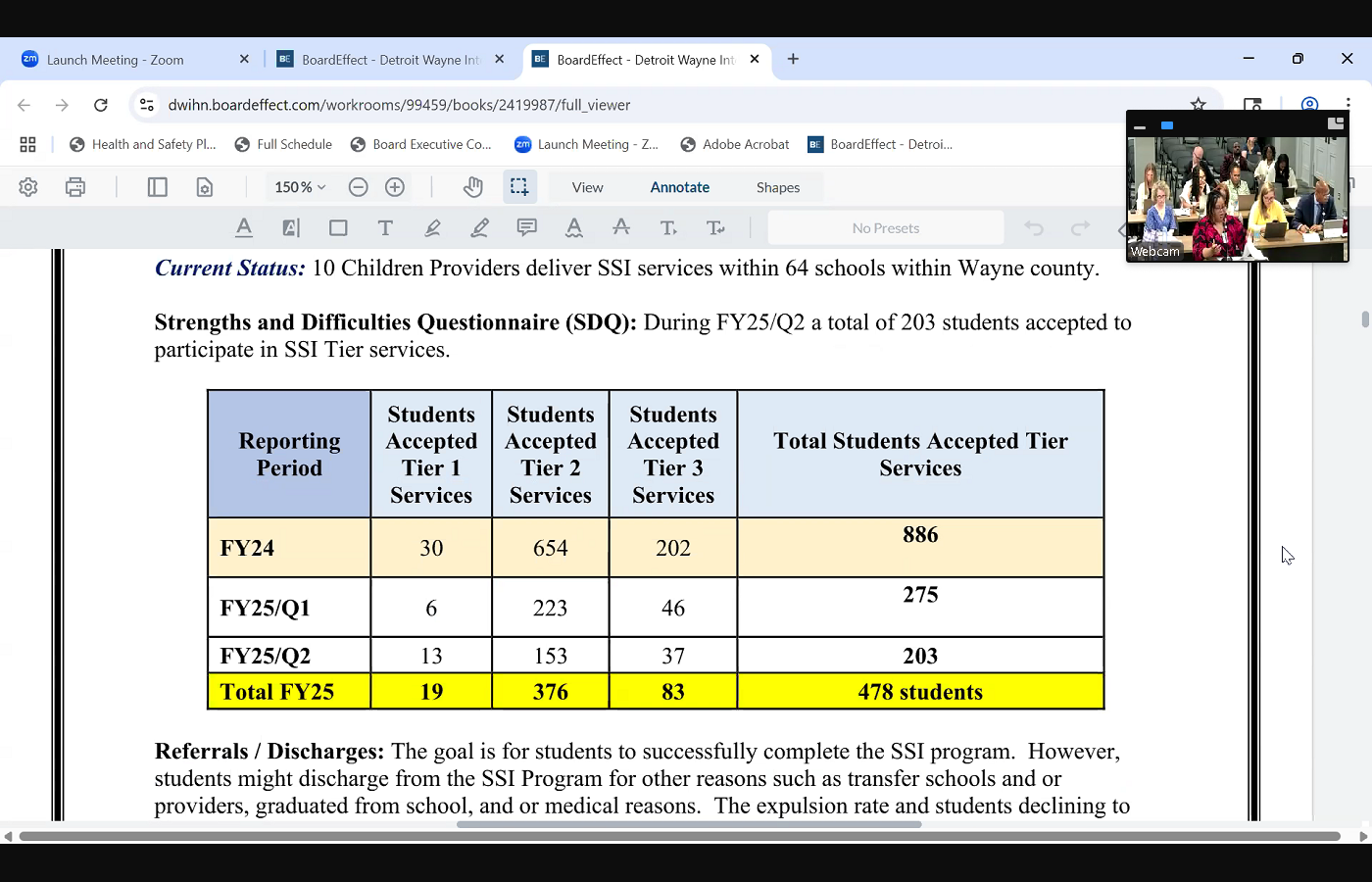
 providers in schools within Wayne County. It's for grades K through 12, and they offer the tier one, tier two and tier three services. They also provide, you know, risk factor presentations and the Michigan model for health curriculum. Some of our goals this year was to develop an integrated health risk factor presentation. We have asthma initiative, completion of the program, reduction in school suspensions and expulsions and reduction in crisis events and hospitalizations. So what happens is, at the beginning of every school year, the therapist administer a strength and difficulties questionnaire, otherwise known as the SDQ. And so as a result of that, for quarter two, there were 203 new students who accepted or agreed to participate in the s the School Success Initiative Program. I want to also inform that when it comes to students being expelled, there were zero students that were expelled during quarter two, and even this entire fiscal year, there were zero expulsions, and there were two that declined to participate in the program. When it comes to crisis screenings and hospitalizations for quarter two, there were three crisis screenings and three youth that were hospitalized. That is a big decrease compared
providers in schools within Wayne County. It's for grades K through 12, and they offer the tier one, tier two and tier three services. They also provide, you know, risk factor presentations and the Michigan model for health curriculum. Some of our goals this year was to develop an integrated health risk factor presentation. We have asthma initiative, completion of the program, reduction in school suspensions and expulsions and reduction in crisis events and hospitalizations. So what happens is, at the beginning of every school year, the therapist administer a strength and difficulties questionnaire, otherwise known as the SDQ. And so as a result of that, for quarter two, there were 203 new students who accepted or agreed to participate in the s the School Success Initiative Program. I want to also inform that when it comes to students being expelled, there were zero students that were expelled during quarter two, and even this entire fiscal year, there were zero expulsions, and there were two that declined to participate in the program. When it comes to crisis screenings and hospitalizations for quarter two, there were three crisis screenings and three youth that were hospitalized. That is a big decrease compared  to fiscal 24 of last year, because last year there were 42 crisis screenings and there were 38 hospitalizations. So we're doing we're seeing a lot of progress this school year with that in that area, we continue to offer risk factor presentations for quarter two, we did a total of 603 presentations, and we continue to monitor our tier services as well. And you know, we work very closely with our Detroit Public School District, because with that district specifically, they have very stringent criteria for those schools, and so we work very closely with them to troubleshoot any, you know, any challenges when it comes to referrals in the schools. And then the last program I want to highlight is the integrated pediatric program. This is a very new program we started in October, and starfish is the provider, and it's really to support pregnant moms and their perinatal health. And so the two goals that we have is the to first increase the access to services for patients that are in OBGYN clinics, and then the second goal is to increase the likelihood of desired outcomes, health outcomes for pregnant mothers. And so starfish has infant mental
to fiscal 24 of last year, because last year there were 42 crisis screenings and there were 38 hospitalizations. So we're doing we're seeing a lot of progress this school year with that in that area, we continue to offer risk factor presentations for quarter two, we did a total of 603 presentations, and we continue to monitor our tier services as well. And you know, we work very closely with our Detroit Public School District, because with that district specifically, they have very stringent criteria for those schools, and so we work very closely with them to troubleshoot any, you know, any challenges when it comes to referrals in the schools. And then the last program I want to highlight is the integrated pediatric program. This is a very new program we started in October, and starfish is the provider, and it's really to support pregnant moms and their perinatal health. And so the two goals that we have is the to first increase the access to services for patients that are in OBGYN clinics, and then the second goal is to increase the likelihood of desired outcomes, health outcomes for pregnant mothers. And so starfish has infant mental 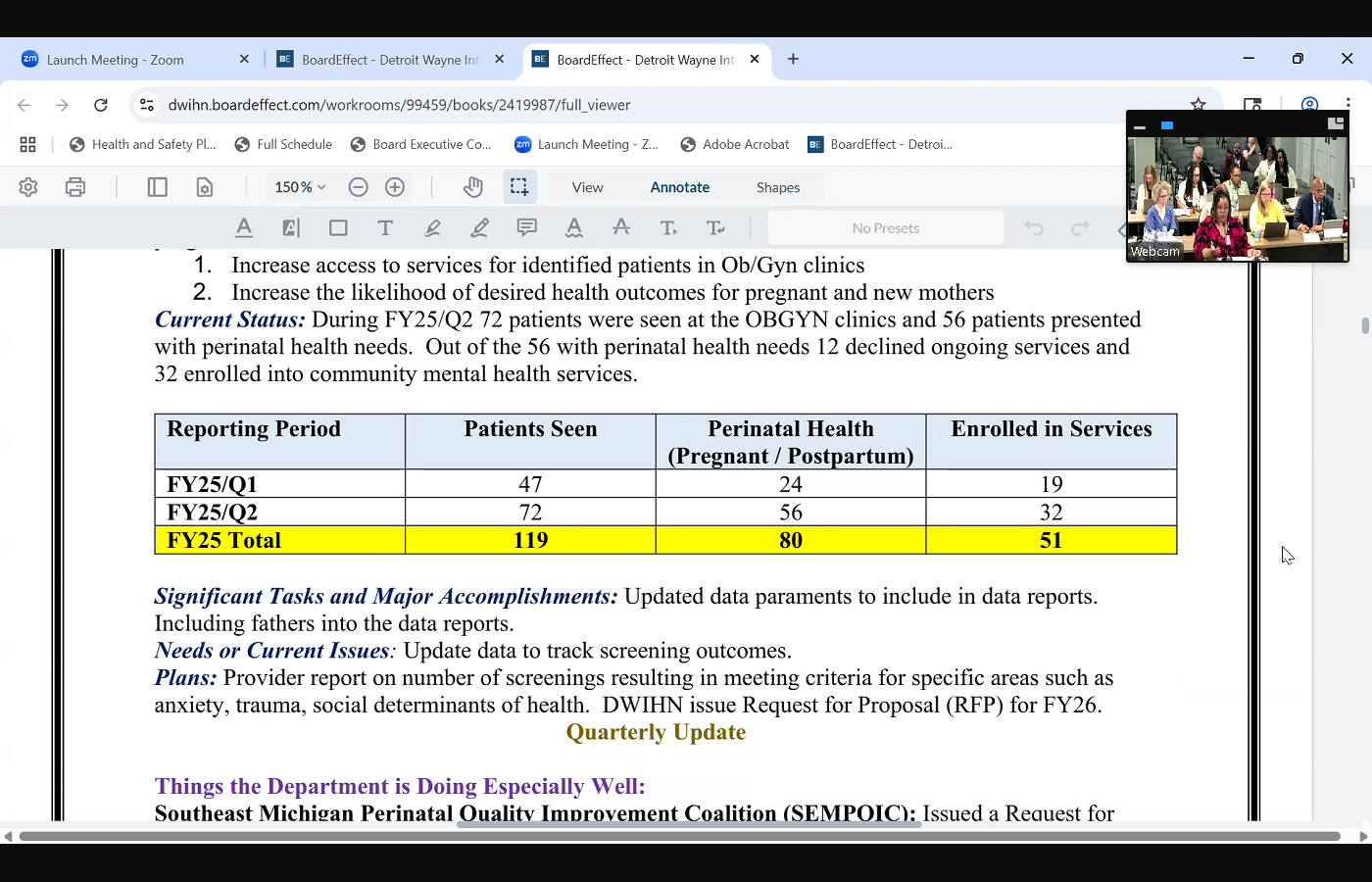
 health therapists in six clinics within Wayne County. They are offering screenings such as anxiety, depression, social determinants of health and trauma to the pregnant moms. And so this fiscal year, as a total, there were 119 patients that were seen. And out of that total, 80 of them presented either with being pregnant or having postpartum depression. And out of that 8051, were enrolled into services. So the goal is to be able to identify the need early on and being able to connect them to services. And so just wanted to share some highlights from the very new the new program that we just launched this year. As far as some updates that occurred during quarter two, we are partnered with SIM quick, which is the Southeast Michigan Perinatal Quality Initiative Coalition. We identify providers that's willing to partner with SIM cramp for a grant to train them on postpartum depression training, and we're partnering with Michigan State University to roll out a new E screening tool so that way those providers that have offered infant mental health services, they're able to do a e screening with those pregnant moms. And so this is a very new pilot program that we're doing this year, and we're excited about it. Also, we will be rolling out a request for proposal RFP for certain programs this year or for next fiscal year. Is the Wayne County Youth, Juvenile Services, autism independent evaluators, the school success program, the goal line program, the pediatric integrated health program, the juvenile restorative program and the hope mobile crisis program. And so we are working on that project. And the last thing I want to inform is we offered wonderful trainings during quarter two, beyond the walls with trauma, signs of suicide, leveraging the power of father engagement, navigating the workplace for new staff as new interns, managing and coaching. And I Lastly, want to share that we have four new members to our team, and two of them are here, Jason Riley and Christine Townsend Dowdell. They oversee our special project specialist for evidence based practices and our school and infant mental health services. So that concludes my report.
health therapists in six clinics within Wayne County. They are offering screenings such as anxiety, depression, social determinants of health and trauma to the pregnant moms. And so this fiscal year, as a total, there were 119 patients that were seen. And out of that total, 80 of them presented either with being pregnant or having postpartum depression. And out of that 8051, were enrolled into services. So the goal is to be able to identify the need early on and being able to connect them to services. And so just wanted to share some highlights from the very new the new program that we just launched this year. As far as some updates that occurred during quarter two, we are partnered with SIM quick, which is the Southeast Michigan Perinatal Quality Initiative Coalition. We identify providers that's willing to partner with SIM cramp for a grant to train them on postpartum depression training, and we're partnering with Michigan State University to roll out a new E screening tool so that way those providers that have offered infant mental health services, they're able to do a e screening with those pregnant moms. And so this is a very new pilot program that we're doing this year, and we're excited about it. Also, we will be rolling out a request for proposal RFP for certain programs this year or for next fiscal year. Is the Wayne County Youth, Juvenile Services, autism independent evaluators, the school success program, the goal line program, the pediatric integrated health program, the juvenile restorative program and the hope mobile crisis program. And so we are working on that project. And the last thing I want to inform is we offered wonderful trainings during quarter two, beyond the walls with trauma, signs of suicide, leveraging the power of father engagement, navigating the workplace for new staff as new interns, managing and coaching. And I Lastly, want to share that we have four new members to our team, and two of them are here, Jason Riley and Christine Townsend Dowdell. They oversee our special project specialist for evidence based practices and our school and infant mental health services. So that concludes my report.
+2
right. So for the quarter two, children's initiatives report, I want to start by just giving an overview of our census here. So for quarter two, we served an average of 13,369 unduplicated children, youth and families in Wayne County. This is for ages zero to their 21st birthday. Also includes those with serious emotional disturbances and intellectual developmental disabilities. This total is slightly higher than the first quarter, and it's also higher than quarter two of last year. And so as of quarter two, the total number is 26,425 so we continue to grow. The three areas that I'm going to focus on today is access to Children Services, the School Success Initiative Program and a new program, which is the pediatric integrated health program. When it comes to access to services, the state of Michigan implemented a new goal for fiscal year 25 that we have to be at 57% for whenever children have a screening completed, that that intake assessment happens within 14 days. This has been an area that we have struggled in over the last year or so, and so I am happy to inform that for quarter two, we were at 62% and which is higher than the 57% goal. There's a lot of efforts that have went into this. Shout out to our quality department and our IT department that helped us, because what we realized was that there were children specialty programs where the children providers were completing screenings, and that was not being factored into our reporting, and so we worked on rolling out a new screening code and including that into the report. And so we were able to reach the goal. The second program I want to highlight is our School Success Initiative Program. This is where we have +5
providers in schools within Wayne County. It's for grades K through 12, and they offer the tier one, tier two and tier three services. They also provide, you know, risk factor presentations and the Michigan model for health curriculum. Some of our goals this year was to develop an integrated health risk factor presentation. We have asthma initiative, completion of the program, reduction in school suspensions and expulsions and reduction in crisis events and hospitalizations. So what happens is, at the beginning of every school year, the therapist administer a strength and difficulties questionnaire, otherwise known as the SDQ. And so as a result of that, for quarter two, there were 203 new students who accepted or agreed to participate in the s the School Success Initiative Program. I want to also inform that when it comes to students being expelled, there were zero students that were expelled during quarter two, and even this entire fiscal year, there were zero expulsions, and there were two that declined to participate in the program. When it comes to crisis screenings and hospitalizations for quarter two, there were three crisis screenings and three youth that were hospitalized. That is a big decrease compared 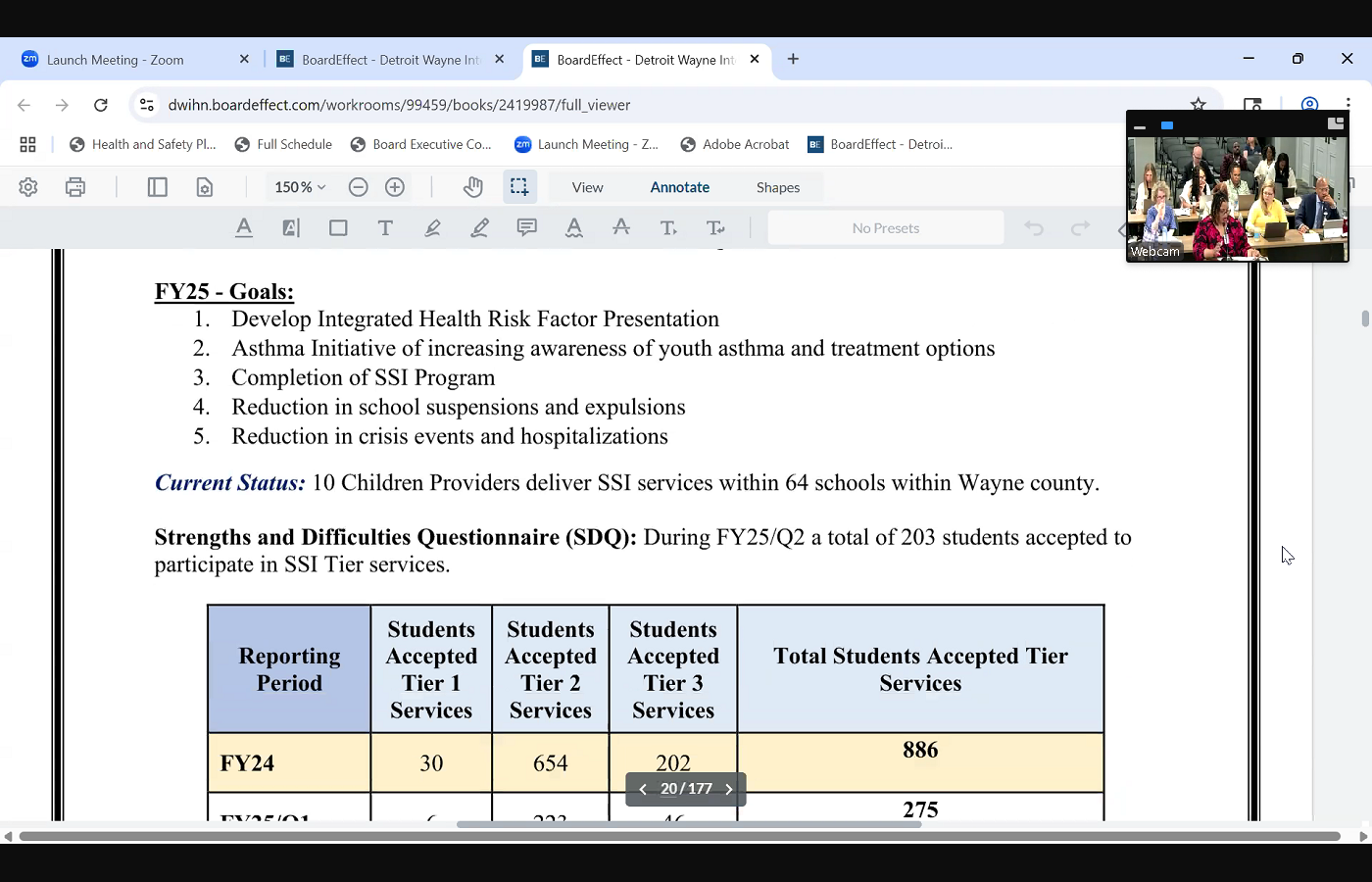

+1
to fiscal 24 of last year, because last year there were 42 crisis screenings and there were 38 hospitalizations. So we're doing we're seeing a lot of progress this school year with that in that area, we continue to offer risk factor presentations for quarter two, we did a total of 603 presentations, and we continue to monitor our tier services as well. And you know, we work very closely with our Detroit Public School District, because with that district specifically, they have very stringent criteria for those schools, and so we work very closely with them to troubleshoot any, you know, any challenges when it comes to referrals in the schools. And then the last program I want to highlight is the integrated pediatric program. This is a very new program we started in October, and starfish is the provider, and it's really to support pregnant moms and their perinatal health. And so the two goals that we have is the to first increase the access to services for patients that are in OBGYN clinics, and then the second goal is to increase the likelihood of desired outcomes, health outcomes for pregnant mothers. And so starfish has infant mental +2
health therapists in six clinics within Wayne County. They are offering screenings such as anxiety, depression, social determinants of health and trauma to the pregnant moms. And so this fiscal year, as a total, there were 119 patients that were seen. And out of that total, 80 of them presented either with being pregnant or having postpartum depression. And out of that 8051, were enrolled into services. So the goal is to be able to identify the need early on and being able to connect them to services. And so just wanted to share some highlights from the very new the new program that we just launched this year. As far as some updates that occurred during quarter two, we are partnered with SIM quick, which is the Southeast Michigan Perinatal Quality Initiative Coalition. We identify providers that's willing to partner with SIM cramp for a grant to train them on postpartum depression training, and we're partnering with Michigan State University to roll out a new E screening tool so that way those providers that have offered infant mental health services, they're able to do a e screening with those pregnant moms. And so this is a very new pilot program that we're doing this year, and we're excited about it. Also, we will be rolling out a request for proposal RFP for certain programs this year or for next fiscal year. Is the Wayne County Youth, Juvenile Services, autism independent evaluators, the school success program, the goal line program, the pediatric integrated health program, the juvenile restorative program and the hope mobile crisis program. And so we are working on that project. And the last thing I want to inform is we offered wonderful trainings during quarter two, beyond the walls with trauma, signs of suicide, leveraging the power of father engagement, navigating the workplace for new staff as new interns, managing and coaching. And I Lastly, want to share that we have four new members to our team, and two of them are here, Jason Riley and Christine Townsend Dowdell. They oversee our special project specialist for evidence based practices and our school and infant mental health services. So that concludes my report. Speaker 2
Thank you for the report. It was chock full of a lot of information. Are there any questions from the member? Yes, I
Speaker 7
don't have a question. I just want to commend you on just an excellent report. Oh, thank you, thorough. I feel like I could see the pictures of what was going on and awesome and a lot of interesting things going on. I look forward to hearing more about some of those initiatives.
Speaker 3
Yes, I'm looking forward to quarter three as well. We have a lot of great things that we can report out on and we have a great team, so we can't do without our team.
Unknown Speaker
Mr. Phillips, any questions?
Speaker 2
I concur, great job. A couple of questions. When you talk about the new program, yes, it's focusing on pregnant moms. Starfish is the provider, and they're looking to identify any behavioral health issues. Is it just for the mom, or do they also include the father of the baby or the soon to be grandmother of the baby? Because both create
Speaker 3
and are part of the behavioral health issues that may develop. Yes, I'm so glad you brought that up, Dr Carter, and I forgot to mention that. So for quarter one, they really weren't including the fathers, and after having that discussion, they did start including that. So for quarter two, they were able to serve as six fathers, so they are starting to include that into their data reporting and outreach to support the fathers as well. That's a great idea to bring up about the grandparents, and I can circle back with them about that to see how they can include that. But yes, we don't want to leave the fathers out of the process, because they can also, you know, experience their own symptoms, you know, throughout the birth age process and afterwards. So thank you for that, but we are including the fathers. How
Speaker 2
far will you follow these members? So once
Speaker 3
they they do their initial screenings, they will refer them to services and get them connected to services. Now I do know that because they're partnering with the clinics, there are some stipulations what they can and can't do when it comes to, like, coordination and, you know, and things like that. There's some barriers in place. But I can definitely circle back to see if they can follow up after someone has been connected to services, just to check to do additional follow up on that. I can look into that further. I
Speaker 2
think that would be powerful, because the true outcome is less with the pregnancy and more with the motherhood. Yes, and many of the girls are even excited because of all the attention they're getting as a soon to be mom, but once she becomes a mom, the excitement ends, the pressure and the difficulty begins, and that's often when all of the support disappears. And so it seems like the true value would be beyond the pregnancy and really start with the delivery going forward for the fathers too.
Speaker 3
Yes, definitely. Yeah, yeah, we'll, we'll look into that further as well. Okay, thank you so much. Thank you all right.
Speaker 2
Moving on. We are at D customer service. You
Speaker 9
Michelle, 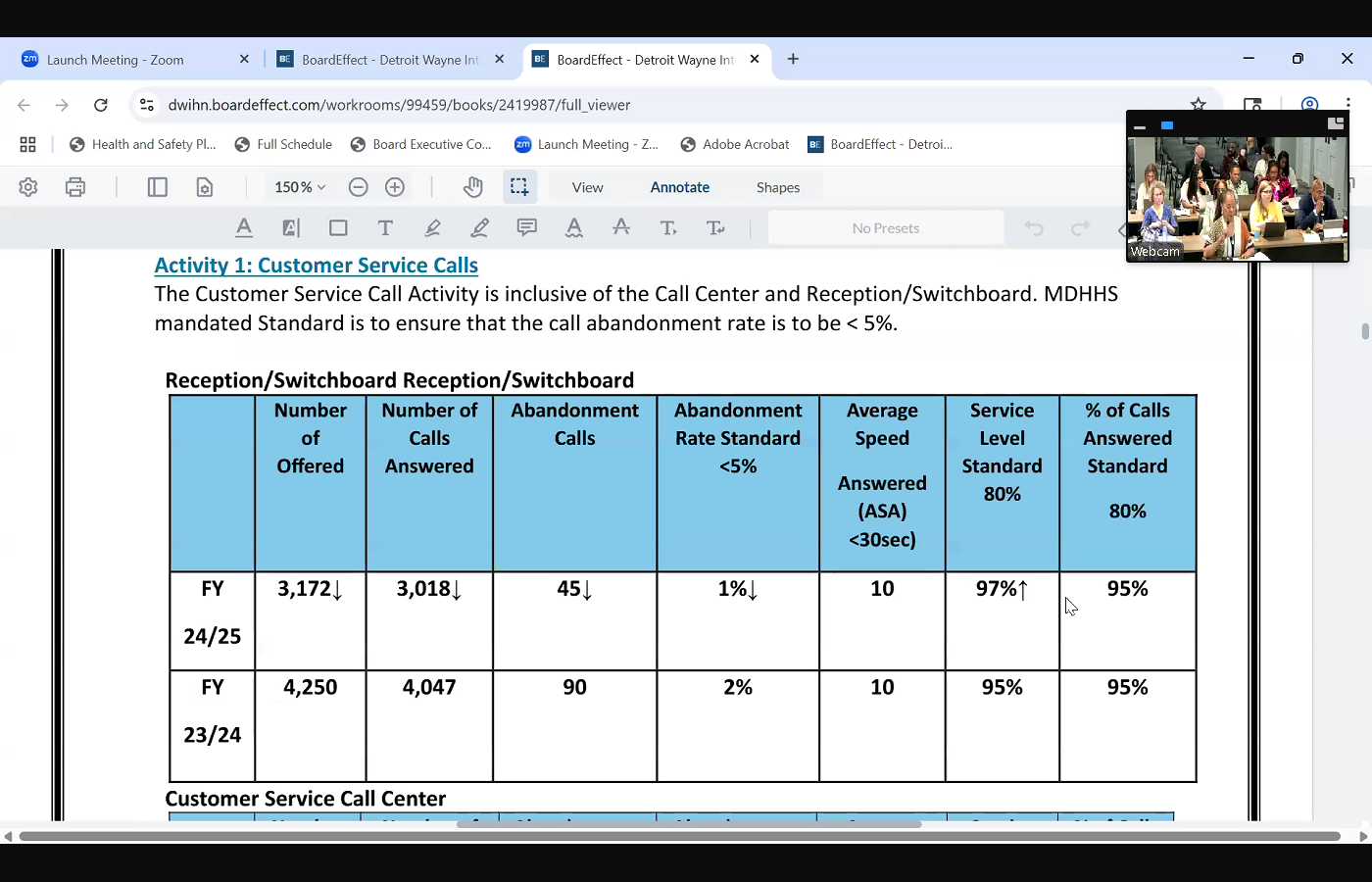
 Good afternoon, Madam Chair and fellow board members. I'm Michelle Vasconcellos. I'm the director of customer service, and my report today will focus on our call center operations, due process and member engagement activities, and this will be for our second quarter. So if you look at our first slide that we have, which is our grid on our switchboard and reception area for the second quarter fiscal year 2324 and 2425 comparison, we did show that there was a decrease in both the number of calls that were offered as well as those that were answered for fiscal year, 2425 there was also a reduction in the number of calls that were abandoned. And our abandonment rate, in fact, reduced down from 2% to 1% and our standard right now is less than 5% for the abandonment rate, so we definitely met that standard. Also our average speed to answer was 10 seconds with a standard of less than 30 seconds. So we've met that standard as well. And so our service level also increased at that time for 90 from 95% to 97% if you look at our second grid, which is actually our customer service call center.
Good afternoon, Madam Chair and fellow board members. I'm Michelle Vasconcellos. I'm the director of customer service, and my report today will focus on our call center operations, due process and member engagement activities, and this will be for our second quarter. So if you look at our first slide that we have, which is our grid on our switchboard and reception area for the second quarter fiscal year 2324 and 2425 comparison, we did show that there was a decrease in both the number of calls that were offered as well as those that were answered for fiscal year, 2425 there was also a reduction in the number of calls that were abandoned. And our abandonment rate, in fact, reduced down from 2% to 1% and our standard right now is less than 5% for the abandonment rate, so we definitely met that standard. Also our average speed to answer was 10 seconds with a standard of less than 30 seconds. So we've met that standard as well. And so our service level also increased at that time for 90 from 95% to 97% if you look at our second grid, which is actually our customer service call center. 
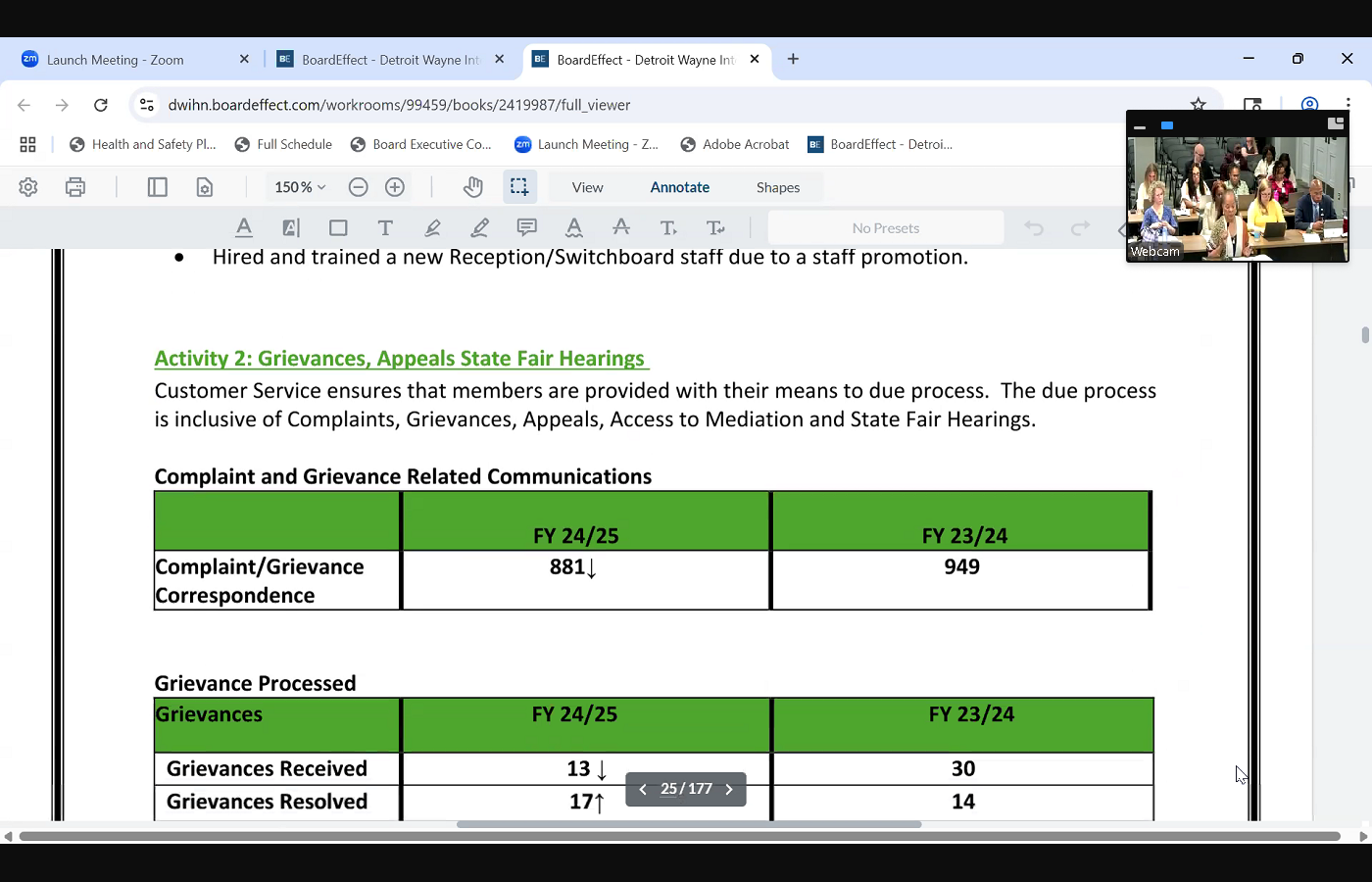 If we compare the data between the two fiscal years, we've seen an increase in both the number of calls that were offered as well as those that were answered in fiscal year 2425 and this kind of reflects our ability to handle rising call traffic, our abandonment rate you found here was at 3% which is again below the standard, as well as our speed to answer was at 10 seconds, and both our service level and percentage of calls that were answered surpassed our 80% standard by achieving an impressive 95% overall. Looking at those these two metrics for both our reception, switchboard and call center, it does illustrate our strong performance and our efforts that we're doing to continue to deliver exceptional call center related services in moving to our next activity, which is our due process. And this first grid focuses on our complaints as well as our grievances related communications, and we did show a decrease in fiscal year 2425 and our second grid also shows us a decrease in the actual grievances that were received in comparison to the previous fiscal year. And we also showed a slight uptick in those grievances that were
If we compare the data between the two fiscal years, we've seen an increase in both the number of calls that were offered as well as those that were answered in fiscal year 2425 and this kind of reflects our ability to handle rising call traffic, our abandonment rate you found here was at 3% which is again below the standard, as well as our speed to answer was at 10 seconds, and both our service level and percentage of calls that were answered surpassed our 80% standard by achieving an impressive 95% overall. Looking at those these two metrics for both our reception, switchboard and call center, it does illustrate our strong performance and our efforts that we're doing to continue to deliver exceptional call center related services in moving to our next activity, which is our due process. And this first grid focuses on our complaints as well as our grievances related communications, and we did show a decrease in fiscal year 2425 and our second grid also shows us a decrease in the actual grievances that were received in comparison to the previous fiscal year. And we also showed a slight uptick in those grievances that were 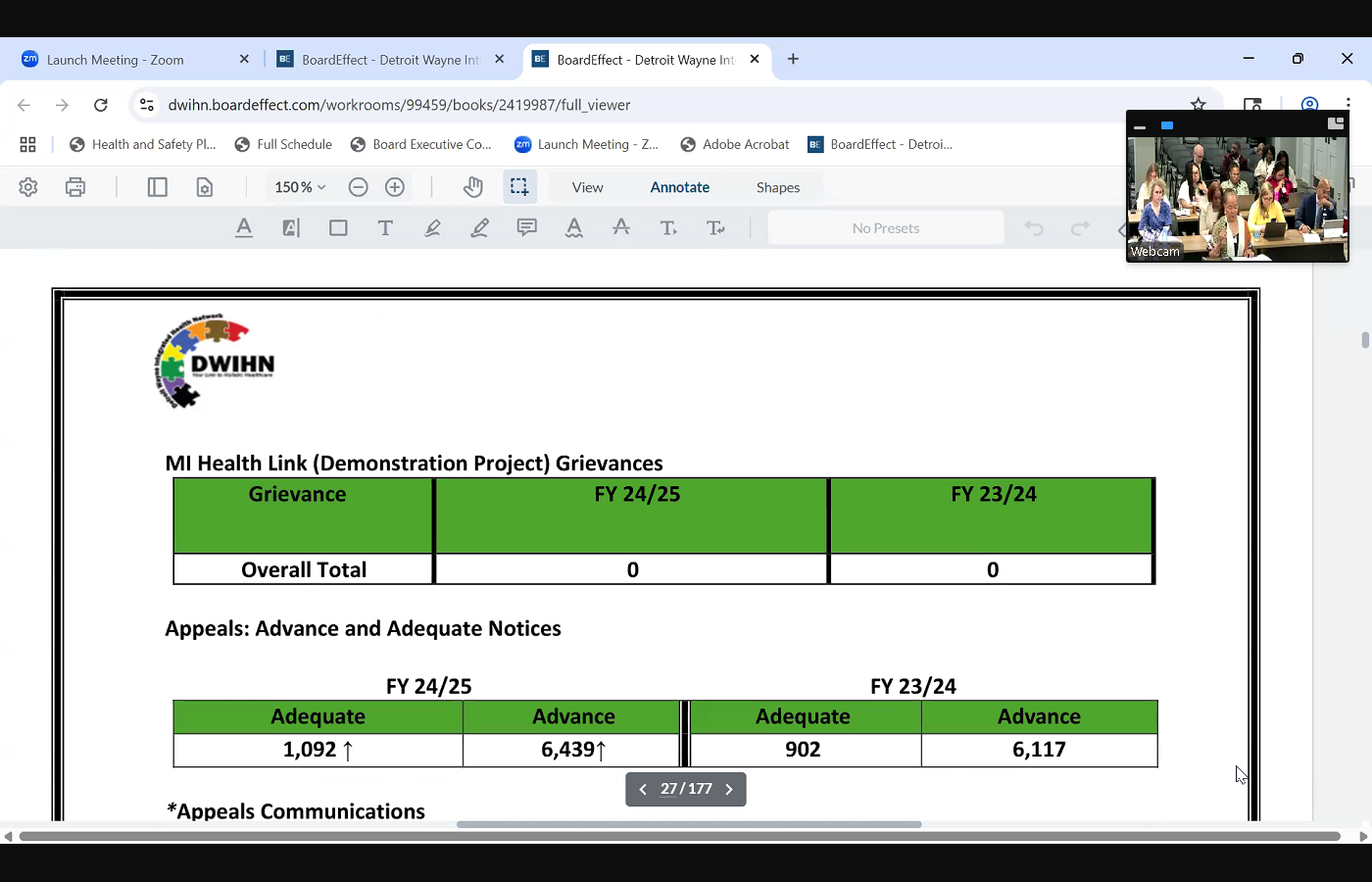
 actually resolved, and that's probably a carry over from the previous quarter. If we look at our our activity in terms of grievances, appeals and state fair hearings, what you'll find is with our complaint and grievance related communications, we did show that there was a decrease, and when we looked at the data, we had gone down from 949 actual communications, which includes letters, fax, telephone conversations that we may have in reference to grievance. It did go down to 881 What you'll also see is that with our our grievances that were actually processed, we showed that there was a significant decrease in those that were actually received, and our grievances for that were resolved. We did show an uptake, an uptake slightly there. If we look at our next grid, you will find that we are looking at our grievances by category. And so as you well know that one particular grievance can actually have several areas of compliance that could be filed in that grievance. And so what we do is we we look at those particular categories, and what you'll notice that we actually had a decrease in the number of grievances for fiscal year
actually resolved, and that's probably a carry over from the previous quarter. If we look at our our activity in terms of grievances, appeals and state fair hearings, what you'll find is with our complaint and grievance related communications, we did show that there was a decrease, and when we looked at the data, we had gone down from 949 actual communications, which includes letters, fax, telephone conversations that we may have in reference to grievance. It did go down to 881 What you'll also see is that with our our grievances that were actually processed, we showed that there was a significant decrease in those that were actually received, and our grievances for that were resolved. We did show an uptake, an uptake slightly there. If we look at our next grid, you will find that we are looking at our grievances by category. And so as you well know that one particular grievance can actually have several areas of compliance that could be filed in that grievance. And so what we do is we we look at those particular categories, and what you'll notice that we actually had a decrease in the number of grievances for fiscal year 
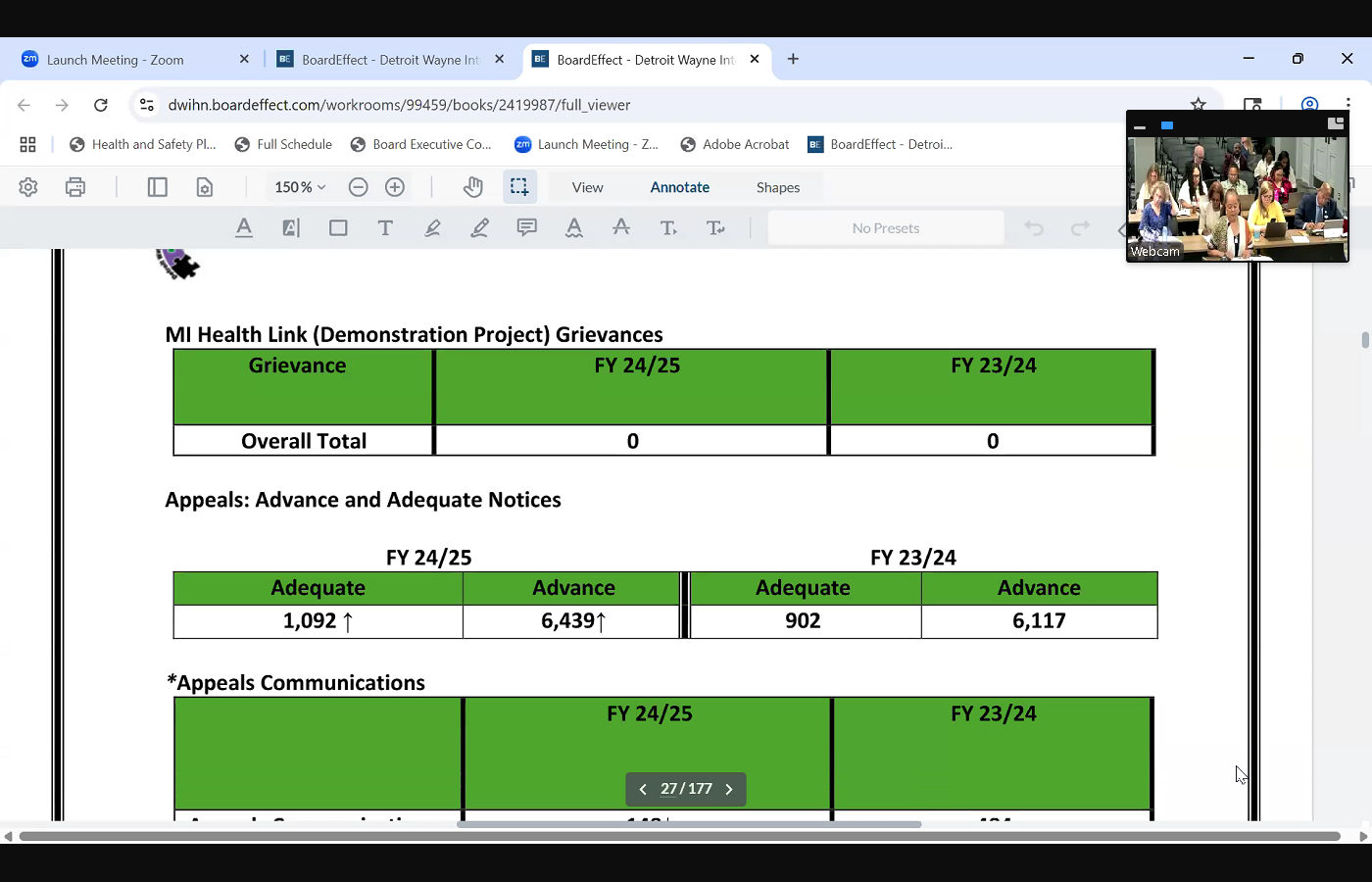 2425 in terms of categories. And so that was a decrease. We had 31 in fiscal year 2425 and fiscal year 2324 we actually showed 57 so we did have a decrease in there. When we looked at our My Health Link program, we actually continue to have zero grievances in that area, and what you'll find is that with our next grid, we actually talk about our appeals in advance and adequate notices. And with our due process area, we monitor samplings of these notices that are generated by our crisp providers, because we want to make sure that our members are provided with the applicable notice as well as the timeliness of that notice. And so with our adequate notices, you're looking at those notices that deny or limit services that are requested and have to go out the same day of the action, whereby the advanced notices it is used to reduce suspender terminate a current notice of our current service, and so these notices have to go out within 10 calendar days of the action. You will note that there was an increase in fiscal year 2425 of both notices that were generated in comparison to
2425 in terms of categories. And so that was a decrease. We had 31 in fiscal year 2425 and fiscal year 2324 we actually showed 57 so we did have a decrease in there. When we looked at our My Health Link program, we actually continue to have zero grievances in that area, and what you'll find is that with our next grid, we actually talk about our appeals in advance and adequate notices. And with our due process area, we monitor samplings of these notices that are generated by our crisp providers, because we want to make sure that our members are provided with the applicable notice as well as the timeliness of that notice. And so with our adequate notices, you're looking at those notices that deny or limit services that are requested and have to go out the same day of the action, whereby the advanced notices it is used to reduce suspender terminate a current notice of our current service, and so these notices have to go out within 10 calendar days of the action. You will note that there was an increase in fiscal year 2425 of both notices that were generated in comparison to 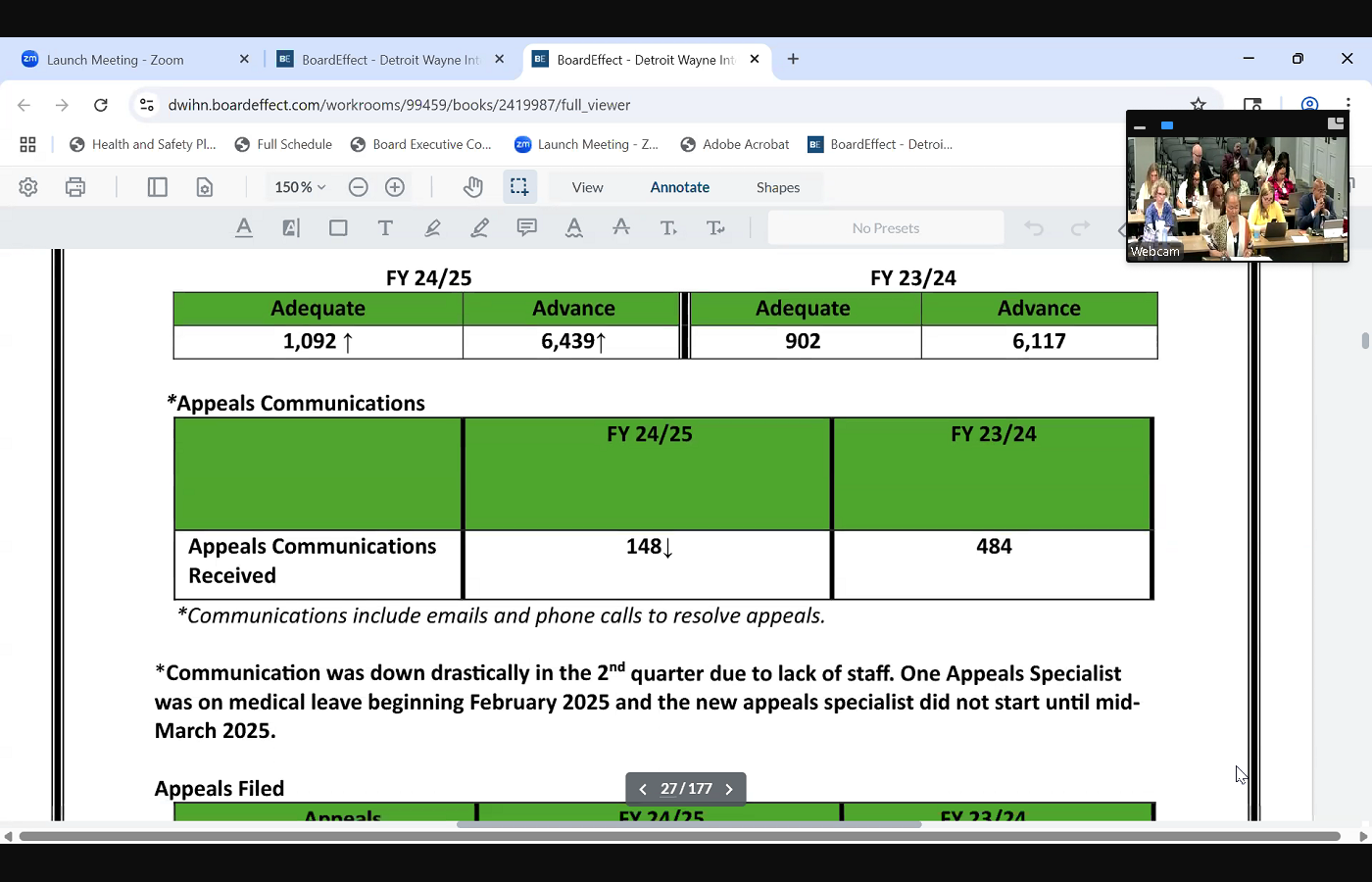
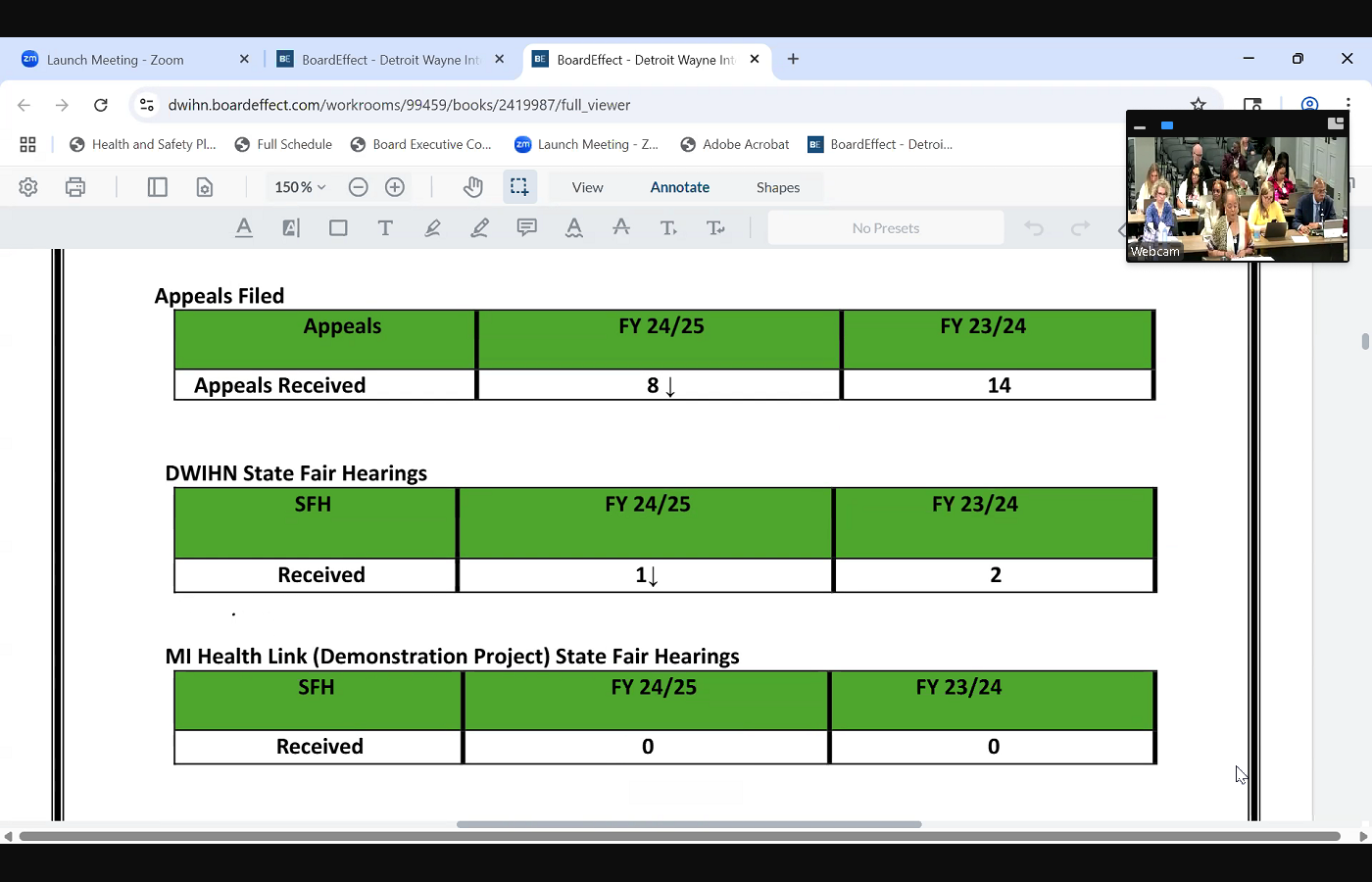 the previous fiscal year, when we go to our appeals and the communications, we did show a significant decrease in those amount of communication efforts. And this was in reference to we did have one appeal specialist that was on medical leave, as well as we also had a vacant position for an appeal specialist. So our staffing was considerably lower at that time, but in March, we were happy to say that we were able to fill the vacant position, and then our person that was on medical leave has just returned back to us this month in our next grid, our appeals that were actually filed, we actually showed that appeals that we received went down slightly from the previous fiscal year. And then our state fair hearings, we actually went down just by one for fiscal year, 2425 and with our demonstration project, which is our My Health Link program, it continues to be at zero. And then if we look at some of the significant activity in the month of March for in reference to our due process area, we did have some competing priorities that needed addressing, which actually involved our disapproval process collaboration, as well as we had one of our autism providers, which was chitter chatter, which was no longer being contracted with us. And so the function of sending out the notices actually was brought in house instead of by our provider. And so that did call for us to have to initiate these notices, which was well over 200 and so that actually took away some of the things that we were doing. But what we did was we also made sure that the things that it affected was not those areas that were a big concern, such as some of our larger trainings that we had initially do throughout the quarter, we kind of subsided on those but we also did some individual trainings and technical assistance to our provider network during that period of time. We also were, as I mentioned, we welcomed a new appeal specialist as well as we continued preparing for our grievance and appeals files, which is our upcoming hsac review, which is going to be this coming Friday. And so we prepared our files for that. And then, as I mentioned, we have been doing also some individual technical assistance with our provider network
the previous fiscal year, when we go to our appeals and the communications, we did show a significant decrease in those amount of communication efforts. And this was in reference to we did have one appeal specialist that was on medical leave, as well as we also had a vacant position for an appeal specialist. So our staffing was considerably lower at that time, but in March, we were happy to say that we were able to fill the vacant position, and then our person that was on medical leave has just returned back to us this month in our next grid, our appeals that were actually filed, we actually showed that appeals that we received went down slightly from the previous fiscal year. And then our state fair hearings, we actually went down just by one for fiscal year, 2425 and with our demonstration project, which is our My Health Link program, it continues to be at zero. And then if we look at some of the significant activity in the month of March for in reference to our due process area, we did have some competing priorities that needed addressing, which actually involved our disapproval process collaboration, as well as we had one of our autism providers, which was chitter chatter, which was no longer being contracted with us. And so the function of sending out the notices actually was brought in house instead of by our provider. And so that did call for us to have to initiate these notices, which was well over 200 and so that actually took away some of the things that we were doing. But what we did was we also made sure that the things that it affected was not those areas that were a big concern, such as some of our larger trainings that we had initially do throughout the quarter, we kind of subsided on those but we also did some individual trainings and technical assistance to our provider network during that period of time. We also were, as I mentioned, we welcomed a new appeal specialist as well as we continued preparing for our grievance and appeals files, which is our upcoming hsac review, which is going to be this coming Friday. And so we prepared our files for that. And then, as I mentioned, we have been doing also some individual technical assistance with our provider network 
 regarding grievances and appeals. Our last item is member engagement and experience. And during our second quarter, we had some some activity that we're kind of proud of. We facilitated February's Valentine's Day soul chat, as well as in March, our member engagement department, we actually sponsored a mental health awareness event. This event focused on expanding resources and opportunities in the community. We did this with a zoom platform, and we showcased various peer panel professionals who spoke on housing, financial literacy, skill building and work opportunities and supported education as well as supported employment. And then we also participated in the review of communications, plan and newsletter condensing, we're looking at some changes to improving our person points of view. Member newsletter, we worked on preparation for our H sag and NCQA requirements from a member engagement aspect. And then we also did our preparation for our spring person points of view newsletter, which actually is going out this month. And then also we started early in terms of preparing for our May Mental Health Awareness Month, and last month, we had a wonderful event here on our campus. And also our CV meetings were moved from our constant center, and we've invited our members to come from our CV to have their meetings here in this facility. Now that ends my report.
regarding grievances and appeals. Our last item is member engagement and experience. And during our second quarter, we had some some activity that we're kind of proud of. We facilitated February's Valentine's Day soul chat, as well as in March, our member engagement department, we actually sponsored a mental health awareness event. This event focused on expanding resources and opportunities in the community. We did this with a zoom platform, and we showcased various peer panel professionals who spoke on housing, financial literacy, skill building and work opportunities and supported education as well as supported employment. And then we also participated in the review of communications, plan and newsletter condensing, we're looking at some changes to improving our person points of view. Member newsletter, we worked on preparation for our H sag and NCQA requirements from a member engagement aspect. And then we also did our preparation for our spring person points of view newsletter, which actually is going out this month. And then also we started early in terms of preparing for our May Mental Health Awareness Month, and last month, we had a wonderful event here on our campus. And also our CV meetings were moved from our constant center, and we've invited our members to come from our CV to have their meetings here in this facility. Now that ends my report.
+2
Good afternoon, Madam Chair and fellow board members. I'm Michelle Vasconcellos. I'm the director of customer service, and my report today will focus on our call center operations, due process and member engagement activities, and this will be for our second quarter. So if you look at our first slide that we have, which is our grid on our switchboard and reception area for the second quarter fiscal year 2324 and 2425 comparison, we did show that there was a decrease in both the number of calls that were offered as well as those that were answered for fiscal year, 2425 there was also a reduction in the number of calls that were abandoned. And our abandonment rate, in fact, reduced down from 2% to 1% and our standard right now is less than 5% for the abandonment rate, so we definitely met that standard. Also our average speed to answer was 10 seconds with a standard of less than 30 seconds. So we've met that standard as well. And so our service level also increased at that time for 90 from 95% to 97% if you look at our second grid, which is actually our customer service call center. +3
If we compare the data between the two fiscal years, we've seen an increase in both the number of calls that were offered as well as those that were answered in fiscal year 2425 and this kind of reflects our ability to handle rising call traffic, our abandonment rate you found here was at 3% which is again below the standard, as well as our speed to answer was at 10 seconds, and both our service level and percentage of calls that were answered surpassed our 80% standard by achieving an impressive 95% overall. Looking at those these two metrics for both our reception, switchboard and call center, it does illustrate our strong performance and our efforts that we're doing to continue to deliver exceptional call center related services in moving to our next activity, which is our due process. And this first grid focuses on our complaints as well as our grievances related communications, and we did show a decrease in fiscal year 2425 and our second grid also shows us a decrease in the actual grievances that were received in comparison to the previous fiscal year. And we also showed a slight uptick in those grievances that were 
+2
actually resolved, and that's probably a carry over from the previous quarter. If we look at our our activity in terms of grievances, appeals and state fair hearings, what you'll find is with our complaint and grievance related communications, we did show that there was a decrease, and when we looked at the data, we had gone down from 949 actual communications, which includes letters, fax, telephone conversations that we may have in reference to grievance. It did go down to 881 What you'll also see is that with our our grievances that were actually processed, we showed that there was a significant decrease in those that were actually received, and our grievances for that were resolved. We did show an uptake, an uptake slightly there. If we look at our next grid, you will find that we are looking at our grievances by category. And so as you well know that one particular grievance can actually have several areas of compliance that could be filed in that grievance. And so what we do is we we look at those particular categories, and what you'll notice that we actually had a decrease in the number of grievances for fiscal year +3
2425 in terms of categories. And so that was a decrease. We had 31 in fiscal year 2425 and fiscal year 2324 we actually showed 57 so we did have a decrease in there. When we looked at our My Health Link program, we actually continue to have zero grievances in that area, and what you'll find is that with our next grid, we actually talk about our appeals in advance and adequate notices. And with our due process area, we monitor samplings of these notices that are generated by our crisp providers, because we want to make sure that our members are provided with the applicable notice as well as the timeliness of that notice. And so with our adequate notices, you're looking at those notices that deny or limit services that are requested and have to go out the same day of the action, whereby the advanced notices it is used to reduce suspender terminate a current notice of our current service, and so these notices have to go out within 10 calendar days of the action. You will note that there was an increase in fiscal year 2425 of both notices that were generated in comparison to 
+3
the previous fiscal year, when we go to our appeals and the communications, we did show a significant decrease in those amount of communication efforts. And this was in reference to we did have one appeal specialist that was on medical leave, as well as we also had a vacant position for an appeal specialist. So our staffing was considerably lower at that time, but in March, we were happy to say that we were able to fill the vacant position, and then our person that was on medical leave has just returned back to us this month in our next grid, our appeals that were actually filed, we actually showed that appeals that we received went down slightly from the previous fiscal year. And then our state fair hearings, we actually went down just by one for fiscal year, 2425 and with our demonstration project, which is our My Health Link program, it continues to be at zero. And then if we look at some of the significant activity in the month of March for in reference to our due process area, we did have some competing priorities that needed addressing, which actually involved our disapproval process collaboration, as well as we had one of our autism providers, which was chitter chatter, which was no longer being contracted with us. And so the function of sending out the notices actually was brought in house instead of by our provider. And so that did call for us to have to initiate these notices, which was well over 200 and so that actually took away some of the things that we were doing. But what we did was we also made sure that the things that it affected was not those areas that were a big concern, such as some of our larger trainings that we had initially do throughout the quarter, we kind of subsided on those but we also did some individual trainings and technical assistance to our provider network during that period of time. We also were, as I mentioned, we welcomed a new appeal specialist as well as we continued preparing for our grievance and appeals files, which is our upcoming hsac review, which is going to be this coming Friday. And so we prepared our files for that. And then, as I mentioned, we have been doing also some individual technical assistance with our provider network 
+2
regarding grievances and appeals. Our last item is member engagement and experience. And during our second quarter, we had some some activity that we're kind of proud of. We facilitated February's Valentine's Day soul chat, as well as in March, our member engagement department, we actually sponsored a mental health awareness event. This event focused on expanding resources and opportunities in the community. We did this with a zoom platform, and we showcased various peer panel professionals who spoke on housing, financial literacy, skill building and work opportunities and supported education as well as supported employment. And then we also participated in the review of communications, plan and newsletter condensing, we're looking at some changes to improving our person points of view. Member newsletter, we worked on preparation for our H sag and NCQA requirements from a member engagement aspect. And then we also did our preparation for our spring person points of view newsletter, which actually is going out this month. And then also we started early in terms of preparing for our May Mental Health Awareness Month, and last month, we had a wonderful event here on our campus. And also our CV meetings were moved from our constant center, and we've invited our members to come from our CV to have their meetings here in this facility. Now that ends my report. Speaker 2
Thank you so much. Excellent. Are there any questions?
Unknown Speaker
Mr. Phillips
Speaker 4
center, yes. And the improvement in numbers, that's a great job. Numbers are very impressive. Thank you. But I do have a question as relates to the overall just a second I'm moving back.
Unknown Speaker
Sorry.
Speaker 10
Hold on. I was a
Speaker 4
number. It was like 1000 less calls received
Unknown Speaker
at the beginning. Are you referring
Unknown Speaker
to the switchboard? Yes, yes.
Unknown Speaker
Is there? Is there any rationale why that's 25%
Unknown Speaker
less calls than were last year.
Speaker 9
So and that kind of surprised us, also, because we we weren't having any difficulties in terms of with fiscal year,
Unknown Speaker
2425 I five
Speaker 9
previous, the previous fiscal year. We know that we had some issues in terms of without Genesis, but we are looking into, we don't seem to understand why we had such a drop. Okay.
Speaker 11
All right, we will look at the calls that were received last year in terms of source of the call, and see if there is a specific section where we see the drop is to your point, and see it could be in absence of known resources, people might be coming to customer service for that advocacy, but at the same time, now that those specific alternate locations have been established, so those calls may have reduced. That could be one argument, but the counter can be, there's a gap in people are aware of that specific survey, so there is a rest utilization. So to your point, we'll certainly look at the data to do some comparisons and provide a feedback at the next PCC, yeah,
Speaker 4
that was more. My concern is such a significant amount of people of less people calling, and maybe there may, you may have had more marketing of the number or something in the past than you did this year, and not as many people are aware. So yeah, I would love to hear more about that. Absolutely. We'll
Unknown Speaker
follow up with that. Thank you.
Speaker 2
Are there any other questions or points, I guess, one question of clarification, when you talk about we met or we exceed the standard of responding to a call within 10 seconds, what does that mean? Does it mean that they are saying, may help you, or are they saying, We know you're waiting, we'll be back.
Speaker 9
I would, I would think that they would say that we're helping them because we're we haven't had a problem in terms of being able to immediately answer that call. So I would, I was think that that would be just curious, because
Speaker 2
so often when people call, that's that first point of them determining the kind of the temperature for the entire encounter, and if someone picks up within 10 seconds, but all they say to me is, there are three people ahead of you. I will be back, versus I'm here to help you. What can I do?
Speaker 9
I think that our history has been that we were able to answer that call and not necessarily have to say that we're going to you're the next number, or we have to put you on hold. I can go back with our supervisor for our call center and and also confirm that, but my understanding is that we haven't had a problem with that
Speaker 4
good thank you. I got one last comment. I, while I understand and appreciate you, know when you speak of call centers to use the term customers, and it kind of bothers me a little bit. So, you know, it's not a big deal, but I think we, you know, the people that are calling are beyond customers, and if we could get some of our creatives to come up with another term that would, that would be great. So that's just the kind of this is my two cents. Do you
Unknown Speaker
have any suggestions? I
Speaker 4
know that's why I say Kim. If we could get our creatives, the creative people in the room, to come up with a different name, I would have a little bit better about it, but I understand that we can't. But still, I just think that the people that are calling are beyond, a little higher level than the customer. So okay,
Speaker 9
and I guess we've kind of, you know, we don't usually like to say that these are members, because the call could be coming from anywhere in our community. And so
Unknown Speaker
thank you. Thank you very much. APPLAUSE,
Speaker 2
you next on our agenda, integrated healthcare.
Unknown Speaker
Good afternoon. Steam board.
Speaker 12
I'm Vicki polotowski Director of integrated care, and I'm here to present, and
Unknown Speaker
I'm having a hard time hearing you.
Speaker 12
Is  that better? Yes, yeah. Okay, let's start over. Good afternoon. Steam board. I'm Vicki polotowski Director of integrated care. The first program I'm going to start on is our obra program, and we are coming on year two of our year over program. Being here at DWIHN and our referrals have stayed about the same per year, about around 100 or 1795
that better? Yes, yeah. Okay, let's start over. Good afternoon. Steam board. I'm Vicki polotowski Director of integrated care. The first program I'm going to start on is our obra program, and we are coming on year two of our year over program. Being here at DWIHN and our referrals have stayed about the same per year, about around 100 or 1795
+1
that better? Yes, yeah. Okay, let's start over. Good afternoon. Steam board. I'm Vicki polotowski Director of integrated care. The first program I'm going to start on is our obra program, and we are coming on year two of our year over program. Being here at DWIHN and our referrals have stayed about the same per year, about around 100 or 1795 Unknown Speaker
we completed 524
Unknown Speaker
full assessments this second quarter, and 166 partial
Speaker 12
that  is an increase of 188 more assessments than last year at that at this time, so we are seeing an increase of people needing assessments being completed, who may be going into the nursing home. We've all done that. We've done that with the same staffing. So we did work with HR to hire three more contingent staff, and we are working with MDHHS right now on a pilot project about how the referrals come to us. Right now, the referrals come to us, and it's just basic information, so our intake specialist then has to then find out all the information, so she has to call the hospitals, the nursing homes, primary care. That takes a lot of time. So we're working with MDHHS now to try to streamline that process where that documentation, documentation is sent over so that we can handle more assessments. So we've we've hired three more contingent staff to help with more assessments. Our second program is complex case management. Our big push in quarter two, we're increasing the referrals and the people who are getting services and complex case management. So we did a lot more focusing on outside agencies to get those referrals, hospitals, primary care offices, substance abuse clinics. And in the end of the first quarter, we started going to our care center to see if going there face to face helped that engagement of people wanting complex case management services. And we saw that out of the 16 new referrals on quarter two. Nine of those were from the care center, and all of those engaged in services. So the care center is a very good going there face to face, presenting to members, and having that time to talk with them is a good intervention. So we're going
is an increase of 188 more assessments than last year at that at this time, so we are seeing an increase of people needing assessments being completed, who may be going into the nursing home. We've all done that. We've done that with the same staffing. So we did work with HR to hire three more contingent staff, and we are working with MDHHS right now on a pilot project about how the referrals come to us. Right now, the referrals come to us, and it's just basic information, so our intake specialist then has to then find out all the information, so she has to call the hospitals, the nursing homes, primary care. That takes a lot of time. So we're working with MDHHS now to try to streamline that process where that documentation, documentation is sent over so that we can handle more assessments. So we've we've hired three more contingent staff to help with more assessments. Our second program is complex case management. Our big push in quarter two, we're increasing the referrals and the people who are getting services and complex case management. So we did a lot more focusing on outside agencies to get those referrals, hospitals, primary care offices, substance abuse clinics. And in the end of the first quarter, we started going to our care center to see if going there face to face helped that engagement of people wanting complex case management services. And we saw that out of the 16 new referrals on quarter two. Nine of those were from the care center, and all of those engaged in services. So the care center is a very good going there face to face, presenting to members, and having that time to talk with them is a good intervention. So we're going 
 to continue, we go every Wednesday to the care center, and then lastly, our HEDIS. So we now have. We've been doing HEDIS for about two years. In quarter two, we hired a HEDIS specialist so she's going to be working with all of our providers, and we sent out letters to all of the providers, of 19 of them who are working with HEDIS, to ask them how their plan was to improve our HEDIS scores, we got all 19 plans back for them from them, and we're working with all of those risk providers to improve those scores. We're also working with a local diabetes clinic and two of our FQHCs to improve diabetes treatment for individuals who are prescribed antipsychotics. That seems to be one that it's hard to get treatment and hard to get that follow up for people, because it's more about just then getting your a 1c checked. It's more about how do you maintain your diabetes? So that's what we're working on right now. Any questions?
to continue, we go every Wednesday to the care center, and then lastly, our HEDIS. So we now have. We've been doing HEDIS for about two years. In quarter two, we hired a HEDIS specialist so she's going to be working with all of our providers, and we sent out letters to all of the providers, of 19 of them who are working with HEDIS, to ask them how their plan was to improve our HEDIS scores, we got all 19 plans back for them from them, and we're working with all of those risk providers to improve those scores. We're also working with a local diabetes clinic and two of our FQHCs to improve diabetes treatment for individuals who are prescribed antipsychotics. That seems to be one that it's hard to get treatment and hard to get that follow up for people, because it's more about just then getting your a 1c checked. It's more about how do you maintain your diabetes? So that's what we're working on right now. Any questions?
+1
is an increase of 188 more assessments than last year at that at this time, so we are seeing an increase of people needing assessments being completed, who may be going into the nursing home. We've all done that. We've done that with the same staffing. So we did work with HR to hire three more contingent staff, and we are working with MDHHS right now on a pilot project about how the referrals come to us. Right now, the referrals come to us, and it's just basic information, so our intake specialist then has to then find out all the information, so she has to call the hospitals, the nursing homes, primary care. That takes a lot of time. So we're working with MDHHS now to try to streamline that process where that documentation, documentation is sent over so that we can handle more assessments. So we've we've hired three more contingent staff to help with more assessments. Our second program is complex case management. Our big push in quarter two, we're increasing the referrals and the people who are getting services and complex case management. So we did a lot more focusing on outside agencies to get those referrals, hospitals, primary care offices, substance abuse clinics. And in the end of the first quarter, we started going to our care center to see if going there face to face helped that engagement of people wanting complex case management services. And we saw that out of the 16 new referrals on quarter two. Nine of those were from the care center, and all of those engaged in services. So the care center is a very good going there face to face, presenting to members, and having that time to talk with them is a good intervention. So we're going +3
to continue, we go every Wednesday to the care center, and then lastly, our HEDIS. So we now have. We've been doing HEDIS for about two years. In quarter two, we hired a HEDIS specialist so she's going to be working with all of our providers, and we sent out letters to all of the providers, of 19 of them who are working with HEDIS, to ask them how their plan was to improve our HEDIS scores, we got all 19 plans back for them from them, and we're working with all of those risk providers to improve those scores. We're also working with a local diabetes clinic and two of our FQHCs to improve diabetes treatment for individuals who are prescribed antipsychotics. That seems to be one that it's hard to get treatment and hard to get that follow up for people, because it's more about just then getting your a 1c checked. It's more about how do you maintain your diabetes? So that's what we're working on right now. Any questions? 
Speaker 2
Other questions? No, this book looks No. Thank you very much. Yeah. So that ends the quarterly reports, and we're going to move on to the presentation Sud initiatives, the E recovery app pilot.
Speaker 13
Hi, 
 good afternoon. Matthew, yes, cold, interim Sud director I'm presenting today on the chess e recovery pilot program. So this the chess app offers a supportive community of individuals in recovery to members at the pilot sites that were chosen. So our participating providers are quality behavioral health and personalized nursing. Lighthouse, the members that enroll in this app can celebrate achievements. They can share strategies to say, stay sober and coping mechanisms, as well as receive support from a peer recovery coach. There is unlimited use by members and alumni at participating provider locations and again, to kind of touch on that peer recovery support that is on demand as well through the app, their current funding for the last two quarters of fiscal year 24 they received 15,000 for all of fiscal year 25 they received 21,000 in total, they have received 36,000 from dwin. So the term for this has been may 2024, through September 30, 2025, when their contract expires. Demographics, by providers. This is utilization by provider, location by age. So as you can see, the majority of individuals enrolled at qbh and personalized nursing are from 31 to 50 years old. There's an interesting
good afternoon. Matthew, yes, cold, interim Sud director I'm presenting today on the chess e recovery pilot program. So this the chess app offers a supportive community of individuals in recovery to members at the pilot sites that were chosen. So our participating providers are quality behavioral health and personalized nursing. Lighthouse, the members that enroll in this app can celebrate achievements. They can share strategies to say, stay sober and coping mechanisms, as well as receive support from a peer recovery coach. There is unlimited use by members and alumni at participating provider locations and again, to kind of touch on that peer recovery support that is on demand as well through the app, their current funding for the last two quarters of fiscal year 24 they received 15,000 for all of fiscal year 25 they received 21,000 in total, they have received 36,000 from dwin. So the term for this has been may 2024, through September 30, 2025, when their contract expires. Demographics, by providers. This is utilization by provider, location by age. So as you can see, the majority of individuals enrolled at qbh and personalized nursing are from 31 to 50 years old. There's an interesting 
 spike of 61 plus at qbh, however, and then gender demographics, the majority we have our mail monthly enrollments by provider. If you look at it just it's peaked during the launching of that in August of 2024 and it has decreased a little bit since a little bit of peaks in enrollment at personalized nursing in January 25 and march 25 as well. I want to talk about escalation. So this is when a member says something in a community post that might be alarming to the chess app folks, when they use a help button saying that they're they need help right away, so a peer recovery coach will reach out, and there is a series of escalation so first, if they push the Help button and they just say, I'm having a craving, they'll get a cognitive behavioral therapy exercise. They'll also get a push notification in the app and a message by a Michigan based peer recovery coach, if needed. After that push notification and in app messaging, they'll get a text message and then a phone call from a peer recovery coach. If for some reason, a text message or phone call aren't answered, they
spike of 61 plus at qbh, however, and then gender demographics, the majority we have our mail monthly enrollments by provider. If you look at it just it's peaked during the launching of that in August of 2024 and it has decreased a little bit since a little bit of peaks in enrollment at personalized nursing in January 25 and march 25 as well. I want to talk about escalation. So this is when a member says something in a community post that might be alarming to the chess app folks, when they use a help button saying that they're they need help right away, so a peer recovery coach will reach out, and there is a series of escalation so first, if they push the Help button and they just say, I'm having a craving, they'll get a cognitive behavioral therapy exercise. They'll also get a push notification in the app and a message by a Michigan based peer recovery coach, if needed. After that push notification and in app messaging, they'll get a text message and then a phone call from a peer recovery coach. If for some reason, a text message or phone call aren't answered, they 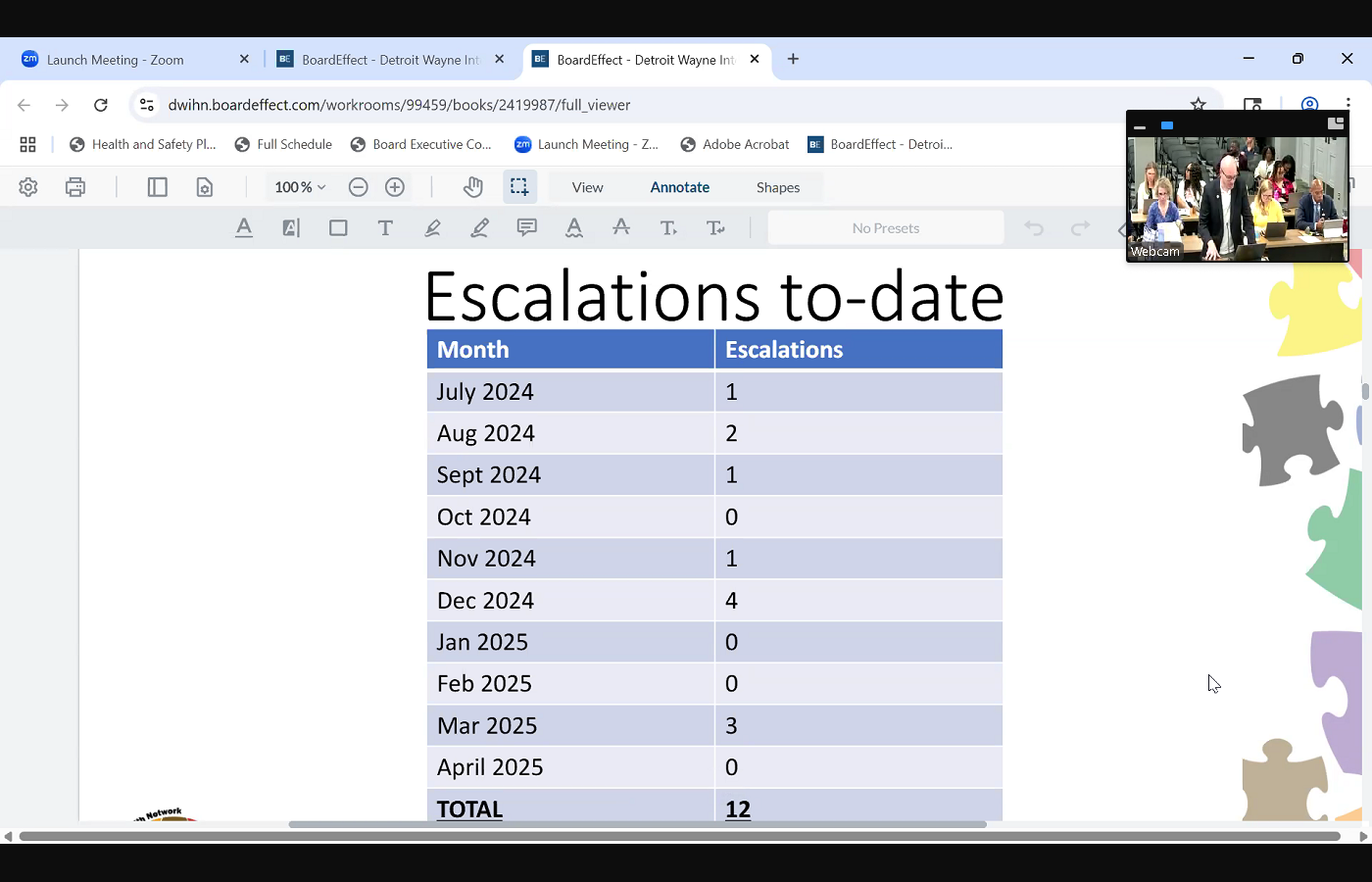
 will place a call to the emergency contacts that are listed in the app, and that hasn't happened yet, but I did ask if the emergency contact didn't respond there, they follow up with communication to the sud. Chris, so escalations to date. There have been 12 escalations to date, and it peaked in December of 2024 we had the most escalations in that month. There were four. A quick drill down at qbh on those escalations. So one was about a concerning community post. One a member reported that they started to use again, and three, they reported in a survey or daily check in that they were not confident in their recovery. Men escalations of personalized nursing. Six reported they weren't confident in their recovery. One that they started using again, and one due to a concerning community post,
will place a call to the emergency contacts that are listed in the app, and that hasn't happened yet, but I did ask if the emergency contact didn't respond there, they follow up with communication to the sud. Chris, so escalations to date. There have been 12 escalations to date, and it peaked in December of 2024 we had the most escalations in that month. There were four. A quick drill down at qbh on those escalations. So one was about a concerning community post. One a member reported that they started to use again, and three, they reported in a survey or daily check in that they were not confident in their recovery. Men escalations of personalized nursing. Six reported they weren't confident in their recovery. One that they started using again, and one due to a concerning community post,
+5
good afternoon. Matthew, yes, cold, interim Sud director I'm presenting today on the chess e recovery pilot program. So this the chess app offers a supportive community of individuals in recovery to members at the pilot sites that were chosen. So our participating providers are quality behavioral health and personalized nursing. Lighthouse, the members that enroll in this app can celebrate achievements. They can share strategies to say, stay sober and coping mechanisms, as well as receive support from a peer recovery coach. There is unlimited use by members and alumni at participating provider locations and again, to kind of touch on that peer recovery support that is on demand as well through the app, their current funding for the last two quarters of fiscal year 24 they received 15,000 for all of fiscal year 25 they received 21,000 in total, they have received 36,000 from dwin. So the term for this has been may 2024, through September 30, 2025, when their contract expires. Demographics, by providers. This is utilization by provider, location by age. So as you can see, the majority of individuals enrolled at qbh and personalized nursing are from 31 to 50 years old. There's an interesting 
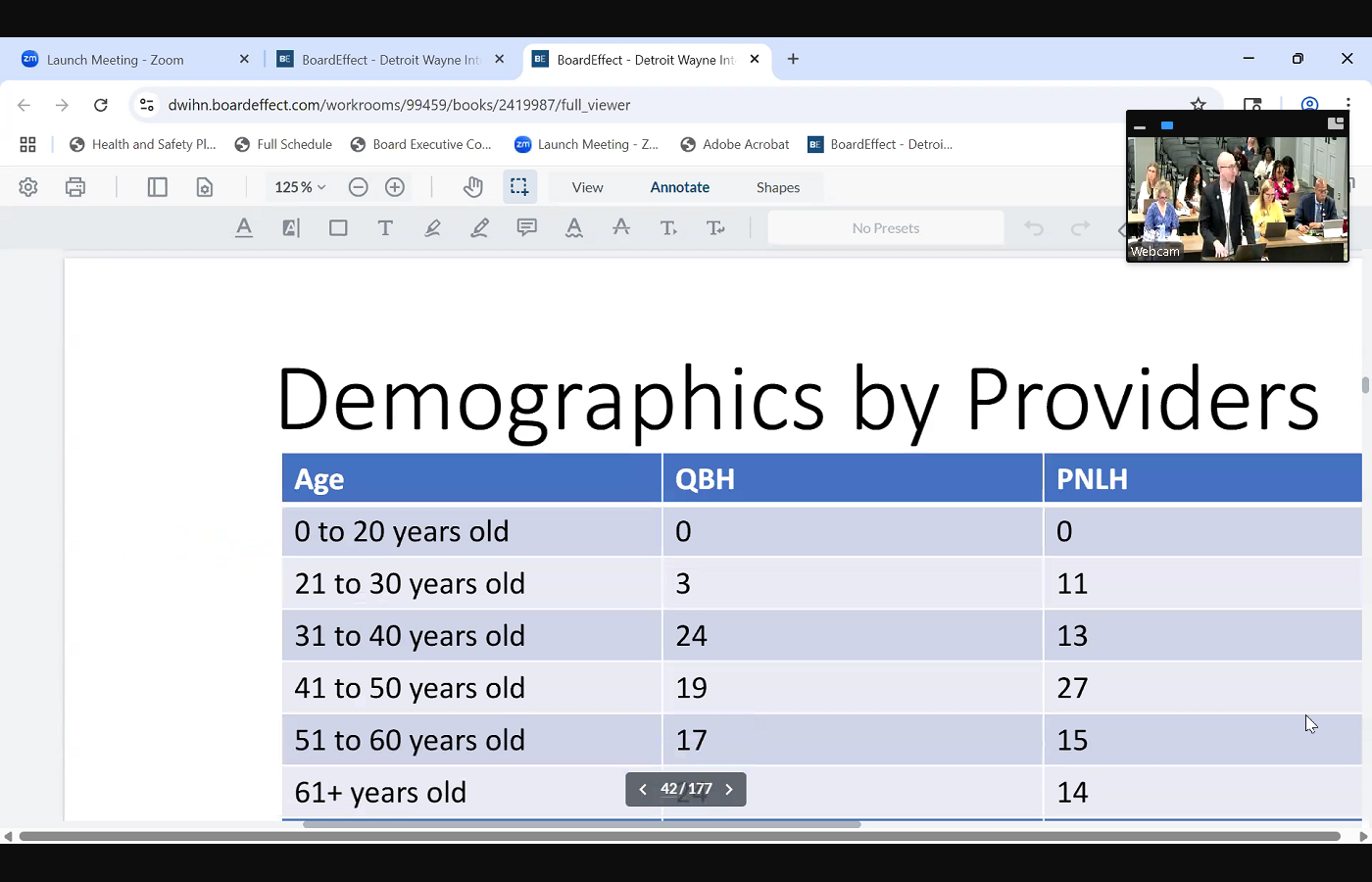

+2
spike of 61 plus at qbh, however, and then gender demographics, the majority we have our mail monthly enrollments by provider. If you look at it just it's peaked during the launching of that in August of 2024 and it has decreased a little bit since a little bit of peaks in enrollment at personalized nursing in January 25 and march 25 as well. I want to talk about escalation. So this is when a member says something in a community post that might be alarming to the chess app folks, when they use a help button saying that they're they need help right away, so a peer recovery coach will reach out, and there is a series of escalation so first, if they push the Help button and they just say, I'm having a craving, they'll get a cognitive behavioral therapy exercise. They'll also get a push notification in the app and a message by a Michigan based peer recovery coach, if needed. After that push notification and in app messaging, they'll get a text message and then a phone call from a peer recovery coach. If for some reason, a text message or phone call aren't answered, they +2
will place a call to the emergency contacts that are listed in the app, and that hasn't happened yet, but I did ask if the emergency contact didn't respond there, they follow up with communication to the sud. Chris, so escalations to date. There have been 12 escalations to date, and it peaked in December of 2024 we had the most escalations in that month. There were four. A quick drill down at qbh on those escalations. So one was about a concerning community post. One a member reported that they started to use again, and three, they reported in a survey or daily check in that they were not confident in their recovery. Men escalations of personalized nursing. Six reported they weren't confident in their recovery. One that they started using again, and one due to a concerning community post, Unknown Speaker
just some quick additional data by the providers. 333
Unknown Speaker
surveys were answered at qeh. 155
Speaker 13
answered  at personalized nursing. Four recovery Help Button utilizations at qeh and one at personalized nursing. And then to touch on in app support. So this is when a peer recovery coach is reaching out and engaging one on one with an individual. The volume for the one on one in app messaging was 133 for SMS or text was 12. And for one on one calls, the volume was 720 minutes in total, and 994
at personalized nursing. Four recovery Help Button utilizations at qeh and one at personalized nursing. And then to touch on in app support. So this is when a peer recovery coach is reaching out and engaging one on one with an individual. The volume for the one on one in app messaging was 133 for SMS or text was 12. And for one on one calls, the volume was 720 minutes in total, and 994
+1
at personalized nursing. Four recovery Help Button utilizations at qeh and one at personalized nursing. And then to touch on in app support. So this is when a peer recovery coach is reaching out and engaging one on one with an individual. The volume for the one on one in app messaging was 133 for SMS or text was 12. And for one on one calls, the volume was 720 minutes in total, and 994 Unknown Speaker
one on one calls.
Speaker 13
So 
 members reported what they enjoyed were recovery date tracking. So the achievements that they get when they progress longitudinally from that recovery date that they put in daily check ins, meetings and libraries, which is the CBT exercises and resources, and then community achievements. So proposed next steps, chess, health was well, first is to build out provider participation, and the next is incorporate contingency management and to dig a little bit deeper into that chess help was chess was contracted by MDHHS to oversee the recovery incentive pilot program, which cash incentivizes members for negative drug screens. We put this in front of the board a couple months back for treatment compliance by contracting with chess for this initiative, chess provides participating beneficiaries with reloadable debit cards, and the clinicians enter objectives achieved, and chest determines incentive applicability, so they provide a layer of risk mitigation to contingency management. So we're exploring implementing that layer of risk mitigation as well into our Sud health home contingency management program as well. So next steps are explore that incorporation and explore incorporating appointment reminders to improve initiation or engagement of alcohol and other drug abuse or dependence treatment. So the IET HEDIS measure and that concludes my report. Thank you.
members reported what they enjoyed were recovery date tracking. So the achievements that they get when they progress longitudinally from that recovery date that they put in daily check ins, meetings and libraries, which is the CBT exercises and resources, and then community achievements. So proposed next steps, chess, health was well, first is to build out provider participation, and the next is incorporate contingency management and to dig a little bit deeper into that chess help was chess was contracted by MDHHS to oversee the recovery incentive pilot program, which cash incentivizes members for negative drug screens. We put this in front of the board a couple months back for treatment compliance by contracting with chess for this initiative, chess provides participating beneficiaries with reloadable debit cards, and the clinicians enter objectives achieved, and chest determines incentive applicability, so they provide a layer of risk mitigation to contingency management. So we're exploring implementing that layer of risk mitigation as well into our Sud health home contingency management program as well. So next steps are explore that incorporation and explore incorporating appointment reminders to improve initiation or engagement of alcohol and other drug abuse or dependence treatment. So the IET HEDIS measure and that concludes my report. Thank you.
+2
members reported what they enjoyed were recovery date tracking. So the achievements that they get when they progress longitudinally from that recovery date that they put in daily check ins, meetings and libraries, which is the CBT exercises and resources, and then community achievements. So proposed next steps, chess, health was well, first is to build out provider participation, and the next is incorporate contingency management and to dig a little bit deeper into that chess help was chess was contracted by MDHHS to oversee the recovery incentive pilot program, which cash incentivizes members for negative drug screens. We put this in front of the board a couple months back for treatment compliance by contracting with chess for this initiative, chess provides participating beneficiaries with reloadable debit cards, and the clinicians enter objectives achieved, and chest determines incentive applicability, so they provide a layer of risk mitigation to contingency management. So we're exploring implementing that layer of risk mitigation as well into our Sud health home contingency management program as well. So next steps are explore that incorporation and explore incorporating appointment reminders to improve initiation or engagement of alcohol and other drug abuse or dependence treatment. So the IET HEDIS measure and that concludes my report. Thank you. Speaker 2
Thank you. It's always interesting to hear how new technology has impact on what we do. Are there any questions?
Unknown Speaker
I just had a couple
Speaker 2
when I look at this app based intervention before the participants were chosen. Did you think about who would best benefit from an app based intervention? Typically, the younger people are more comfortable or more app pliable. You have to be literate, you have to have a phone. So were there any exclusions for those who could not participate? That
Speaker 13
is a very good question, and I do agree, and it's interesting too. You know, when we look at demographics, that it's older adults that are utilizing it. To my knowledge, when the pilot providers were procured, it was by interest, not by an assessment of of of members that would most engage well with that, but that's as we look into building it out, I think that's a great thing to consider,
Speaker 2
yeah, because interest doesn't always equal need, right? And with that in mind, you talked about escalations and there being a recovery Help button, and that would lead to a CBT exercise. Yes, is that exercise one for all, because when you provided the demographics, I was really struck by less the age. But outcome is so typically dependent upon the length of use. And if someone is has been using for 25 years, their outcome will be different than someone who's been using for three years if given the same intervention. So I'm wondering if there was any calculus with that in mind,
Unknown Speaker
right? Yes. So the question
Speaker 13
is, is the CBT exercise boilerplate? Yes, or does it refine it a little bit more based on maybe the way that the member responded in surveys, or length
Speaker 2
of use, number of, you know, failed recovery attempts, etc. Can I
Unknown Speaker
get back to you on that?
Speaker 2
Thank you. Would you have a question? Miss below, okay, we're done. We really appreciate that. Thanks. Thank you. I'm on the mic. Un program. Description, executive summary, good
Speaker 14
afternoon. 
 Marlena Hampton, Director of utilization management, with an executive summary of our program description for fiscal years 25 through 27 so I will be brief. Obviously, utilization management functions are guided by our being good stewards of Medicaid dollars and obviously doing providing effective, consistent and high quality services that lead to positive financial outcomes. So I will not bore you with the purpose of our un program, but just know that again, it focuses on making sure that we have processes and that align with the strategic plan as identified by the board. Our scope again, is to make sure that our core to manage our core functions, which would be pre service, concurrent and post service reviews, denials and appeals, discharge planning, monitoring of overall network service utilization and other care management activities. But for the piece that I'm here for and asking for approval of, there are some required revisions and additions to our program description, beginning with our CCBHC requirements for utilization management. So per the CCBHC handbook, pihp, utilization management departments are doing limited retrospective review of approved services to confirm that care was medically necessary. So that is required to be listed in our documentation. Additionally, though, it's not a new element, it's actually which is an oversight in our previous program description, we found that we lacked a statement saying that expedited decisions must be made within 72 hours after receiving that request for service. So again, that is present in all of all of our other policies and procedures, but somehow was overlooked in the program description. So we have added that Additionally, as I've mentioned during our program evaluation, and also in other monthly reporting, we are coming up on needing to add the additional health equity analysis piece to our program description and our program in general. So we're going to be conducting an annual health equity analysis of prior authorization policies and procedures, as indicated by the Centers for Medicare and Medicaid. Finally, some changes recommended and approved by the U M committee. So the updated job description. So we're looking to streamline the job descriptions as listed. Essentially, it looks like they were copied and pasted without really focusing on details related to the utilization management scope. So we're making sure that we only include what's necessary, and also updating some job titles and removing any obsolete positions and the lastly, we were talking about the derivation of u m department goals. So it seemed, for lack of a better word, a bit clunky, to way we were using our utilizing goals before. So we've removed the non essential, essential requirement of program goals being derived directly from the strategic plan. While everything we do works in service of the strategic plan, it makes more sense that our goals are aligned with our department's purpose and daily function, so that way, it actually more closely informs our annual evaluation. And so I am seeking approval from this body to move this on to the full board, Move for approval.
Marlena Hampton, Director of utilization management, with an executive summary of our program description for fiscal years 25 through 27 so I will be brief. Obviously, utilization management functions are guided by our being good stewards of Medicaid dollars and obviously doing providing effective, consistent and high quality services that lead to positive financial outcomes. So I will not bore you with the purpose of our un program, but just know that again, it focuses on making sure that we have processes and that align with the strategic plan as identified by the board. Our scope again, is to make sure that our core to manage our core functions, which would be pre service, concurrent and post service reviews, denials and appeals, discharge planning, monitoring of overall network service utilization and other care management activities. But for the piece that I'm here for and asking for approval of, there are some required revisions and additions to our program description, beginning with our CCBHC requirements for utilization management. So per the CCBHC handbook, pihp, utilization management departments are doing limited retrospective review of approved services to confirm that care was medically necessary. So that is required to be listed in our documentation. Additionally, though, it's not a new element, it's actually which is an oversight in our previous program description, we found that we lacked a statement saying that expedited decisions must be made within 72 hours after receiving that request for service. So again, that is present in all of all of our other policies and procedures, but somehow was overlooked in the program description. So we have added that Additionally, as I've mentioned during our program evaluation, and also in other monthly reporting, we are coming up on needing to add the additional health equity analysis piece to our program description and our program in general. So we're going to be conducting an annual health equity analysis of prior authorization policies and procedures, as indicated by the Centers for Medicare and Medicaid. Finally, some changes recommended and approved by the U M committee. So the updated job description. So we're looking to streamline the job descriptions as listed. Essentially, it looks like they were copied and pasted without really focusing on details related to the utilization management scope. So we're making sure that we only include what's necessary, and also updating some job titles and removing any obsolete positions and the lastly, we were talking about the derivation of u m department goals. So it seemed, for lack of a better word, a bit clunky, to way we were using our utilizing goals before. So we've removed the non essential, essential requirement of program goals being derived directly from the strategic plan. While everything we do works in service of the strategic plan, it makes more sense that our goals are aligned with our department's purpose and daily function, so that way, it actually more closely informs our annual evaluation. And so I am seeking approval from this body to move this on to the full board, Move for approval.
+2
Marlena Hampton, Director of utilization management, with an executive summary of our program description for fiscal years 25 through 27 so I will be brief. Obviously, utilization management functions are guided by our being good stewards of Medicaid dollars and obviously doing providing effective, consistent and high quality services that lead to positive financial outcomes. So I will not bore you with the purpose of our un program, but just know that again, it focuses on making sure that we have processes and that align with the strategic plan as identified by the board. Our scope again, is to make sure that our core to manage our core functions, which would be pre service, concurrent and post service reviews, denials and appeals, discharge planning, monitoring of overall network service utilization and other care management activities. But for the piece that I'm here for and asking for approval of, there are some required revisions and additions to our program description, beginning with our CCBHC requirements for utilization management. So per the CCBHC handbook, pihp, utilization management departments are doing limited retrospective review of approved services to confirm that care was medically necessary. So that is required to be listed in our documentation. Additionally, though, it's not a new element, it's actually which is an oversight in our previous program description, we found that we lacked a statement saying that expedited decisions must be made within 72 hours after receiving that request for service. So again, that is present in all of all of our other policies and procedures, but somehow was overlooked in the program description. So we have added that Additionally, as I've mentioned during our program evaluation, and also in other monthly reporting, we are coming up on needing to add the additional health equity analysis piece to our program description and our program in general. So we're going to be conducting an annual health equity analysis of prior authorization policies and procedures, as indicated by the Centers for Medicare and Medicaid. Finally, some changes recommended and approved by the U M committee. So the updated job description. So we're looking to streamline the job descriptions as listed. Essentially, it looks like they were copied and pasted without really focusing on details related to the utilization management scope. So we're making sure that we only include what's necessary, and also updating some job titles and removing any obsolete positions and the lastly, we were talking about the derivation of u m department goals. So it seemed, for lack of a better word, a bit clunky, to way we were using our utilizing goals before. So we've removed the non essential, essential requirement of program goals being derived directly from the strategic plan. While everything we do works in service of the strategic plan, it makes more sense that our goals are aligned with our department's purpose and daily function, so that way, it actually more closely informs our annual evaluation. And so I am seeking approval from this body to move this on to the full board, Move for approval. Speaker 2
All those in favor, please say Aye, Aye, nays or abstentions. Report approved. Thank you. You're welcome, and thank you.
Speaker 2
Strategic Plan, there's no report, and now we'll move on to quality reviews. Yeah, you're already ready. I'm ready. Yes,
Speaker 4
such a good summary that it would be great to, like, get a summary on each department like that, so that we could, like, really know in detail what each department does. I mean, that was like, when she came up there, I was like, You, she's actually wasting her time. I've read this. She's, you know, it's so clear what they do. So
Unknown Speaker
it would be great to have something like that. Awesome.
Unknown Speaker
Thank you. I'm not saying she should do them all, but
Unknown Speaker
everybody looking at her like
Speaker 2
I think she should. I think that reflects that each area does so much, yes, and that's the nice to capture it in a document, just reminders of how much and then see the interconnectedness. So yes, that's true. Thank
Speaker 15
you. 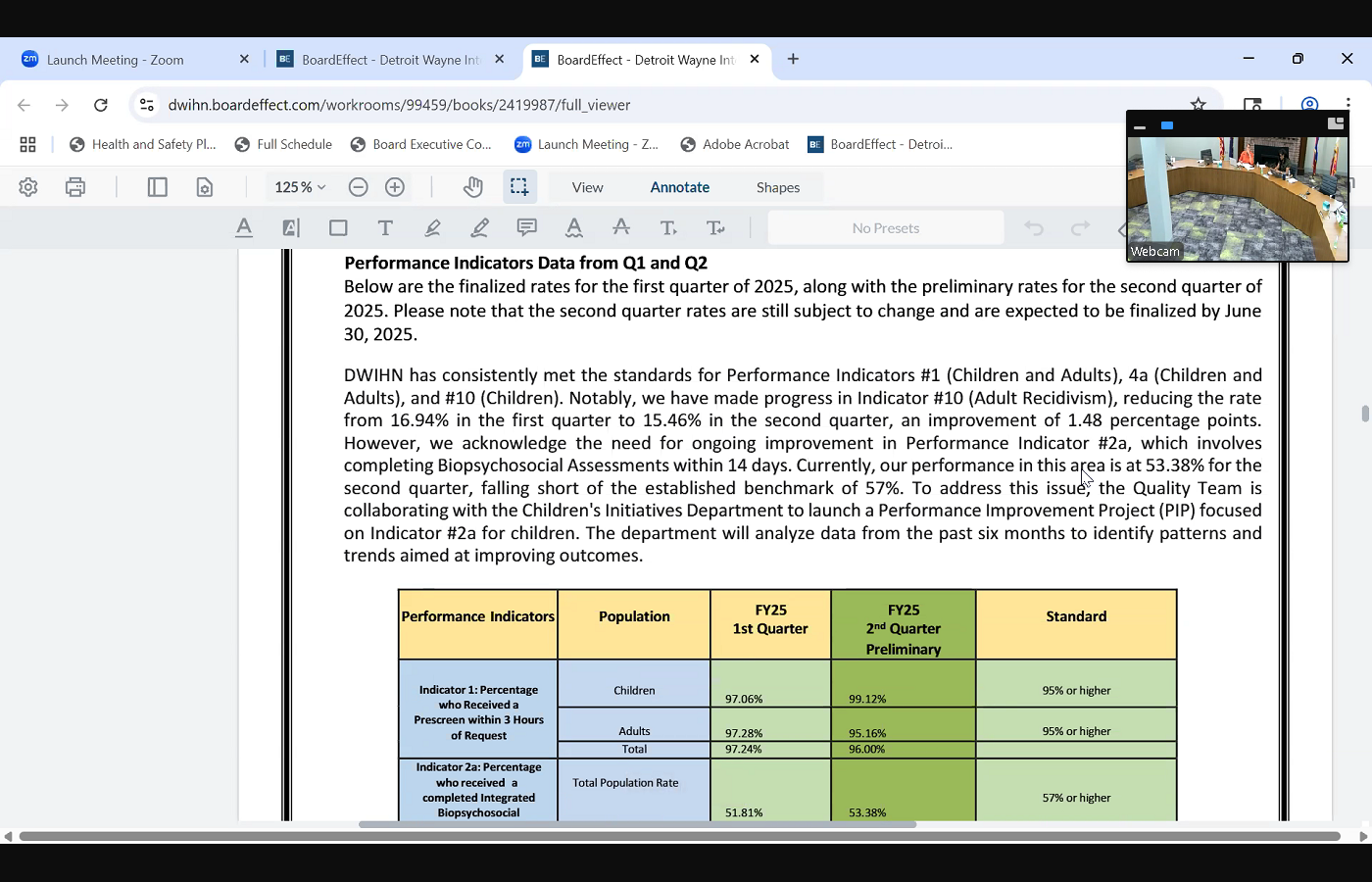
 Good afternoon, Madam Chair, distinguished board members. April Seaver, Director of Quality Improvement, I will I too will be brief. I'm just going to provide you with an overview of our performance indicator data for quarter one and quarter two as a system. How we doing as a system, as you can see in the report below is our finalized rates for first quarter, along with our preliminary rates for second quarter of fiscal year 25 please keep in mind that second quarter rates are still subject to change, and they're not expected to be finalized until June 30, but this just gives you a pretty much snapshot as to where we are at this moment, just real quickly. As you can see, dwin has consistently performed strong in meeting our standards for performance indicator, one, children and adults for four, a children and adults and pi 10 children. Notably, I do want to acknowledge that we have made progress with indicator 10 adult recidivism, reducing the rate from 16.94 in the first quarter to 15.46 in the second quarter, an improvement of 1.48 percentage points. So it tells us what we're doing is working, so we're going to continue with our efforts on that end, as you heard during the presentation today, regarding our two a we acknowledge that we still have more work to do, but we have made significant progress in moving towards meeting that standard. One of the things that we did not or we failed to mention, is that we are the quality team will be collaborating with the children initiative department to launch a performance improvement project where we can focus more on to a and aim at those children and kind of do a deeper dive at the data for the past six
Good afternoon, Madam Chair, distinguished board members. April Seaver, Director of Quality Improvement, I will I too will be brief. I'm just going to provide you with an overview of our performance indicator data for quarter one and quarter two as a system. How we doing as a system, as you can see in the report below is our finalized rates for first quarter, along with our preliminary rates for second quarter of fiscal year 25 please keep in mind that second quarter rates are still subject to change, and they're not expected to be finalized until June 30, but this just gives you a pretty much snapshot as to where we are at this moment, just real quickly. As you can see, dwin has consistently performed strong in meeting our standards for performance indicator, one, children and adults for four, a children and adults and pi 10 children. Notably, I do want to acknowledge that we have made progress with indicator 10 adult recidivism, reducing the rate from 16.94 in the first quarter to 15.46 in the second quarter, an improvement of 1.48 percentage points. So it tells us what we're doing is working, so we're going to continue with our efforts on that end, as you heard during the presentation today, regarding our two a we acknowledge that we still have more work to do, but we have made significant progress in moving towards meeting that standard. One of the things that we did not or we failed to mention, is that we are the quality team will be collaborating with the children initiative department to launch a performance improvement project where we can focus more on to a and aim at those children and kind of do a deeper dive at the data for the past six 
 months to Identify any patterns or trends that will help us improve our outcomes. So that just gives you a quick snapshot of our performance indicator data as a system real quickly. I do want to mention that we are it's that time of year where DWIHN is approaching our external quality reviews. All the pihps across the state goes through these reviews annually. We are scheduled to go through our external quality review where they will it's called our compliance review, where they will evaluate our operation in the following areas that review is scheduled to take place on June 13. And I must say that we are prepared. We are ready. As you can see, I highlighted our previous year performance and how we did. This is a three year review. The first year, there's 13 standards that are part of this review. The first year, they review six, and this year they're going to review the remaining eight. And as you can see, in our strengths, I did want to highlight because I think it's important to know that our score improves substantially. In fact, we were third among all the pihps in the state in terms of our score for the first year. So I'm excited about that. So I'm going to stop right there and entertain any questions that you may have. Oh, and one more thing I do want to mention that it's my hope in September that I can give you some data on our performance monitoring metrics, the quality teams right now as we, as I speak, is out there monitoring our system, and I'm hoping to bring some of that information back to You, hopefully in September, when we get all the information and analyze all the data and whatnot. Thank you. Thank
months to Identify any patterns or trends that will help us improve our outcomes. So that just gives you a quick snapshot of our performance indicator data as a system real quickly. I do want to mention that we are it's that time of year where DWIHN is approaching our external quality reviews. All the pihps across the state goes through these reviews annually. We are scheduled to go through our external quality review where they will it's called our compliance review, where they will evaluate our operation in the following areas that review is scheduled to take place on June 13. And I must say that we are prepared. We are ready. As you can see, I highlighted our previous year performance and how we did. This is a three year review. The first year, there's 13 standards that are part of this review. The first year, they review six, and this year they're going to review the remaining eight. And as you can see, in our strengths, I did want to highlight because I think it's important to know that our score improves substantially. In fact, we were third among all the pihps in the state in terms of our score for the first year. So I'm excited about that. So I'm going to stop right there and entertain any questions that you may have. Oh, and one more thing I do want to mention that it's my hope in September that I can give you some data on our performance monitoring metrics, the quality teams right now as we, as I speak, is out there monitoring our system, and I'm hoping to bring some of that information back to You, hopefully in September, when we get all the information and analyze all the data and whatnot. Thank you. Thank
+2
Good afternoon, Madam Chair, distinguished board members. April Seaver, Director of Quality Improvement, I will I too will be brief. I'm just going to provide you with an overview of our performance indicator data for quarter one and quarter two as a system. How we doing as a system, as you can see in the report below is our finalized rates for first quarter, along with our preliminary rates for second quarter of fiscal year 25 please keep in mind that second quarter rates are still subject to change, and they're not expected to be finalized until June 30, but this just gives you a pretty much snapshot as to where we are at this moment, just real quickly. As you can see, dwin has consistently performed strong in meeting our standards for performance indicator, one, children and adults for four, a children and adults and pi 10 children. Notably, I do want to acknowledge that we have made progress with indicator 10 adult recidivism, reducing the rate from 16.94 in the first quarter to 15.46 in the second quarter, an improvement of 1.48 percentage points. So it tells us what we're doing is working, so we're going to continue with our efforts on that end, as you heard during the presentation today, regarding our two a we acknowledge that we still have more work to do, but we have made significant progress in moving towards meeting that standard. One of the things that we did not or we failed to mention, is that we are the quality team will be collaborating with the children initiative department to launch a performance improvement project where we can focus more on to a and aim at those children and kind of do a deeper dive at the data for the past six +2
months to Identify any patterns or trends that will help us improve our outcomes. So that just gives you a quick snapshot of our performance indicator data as a system real quickly. I do want to mention that we are it's that time of year where DWIHN is approaching our external quality reviews. All the pihps across the state goes through these reviews annually. We are scheduled to go through our external quality review where they will it's called our compliance review, where they will evaluate our operation in the following areas that review is scheduled to take place on June 13. And I must say that we are prepared. We are ready. As you can see, I highlighted our previous year performance and how we did. This is a three year review. The first year, there's 13 standards that are part of this review. The first year, they review six, and this year they're going to review the remaining eight. And as you can see, in our strengths, I did want to highlight because I think it's important to know that our score improves substantially. In fact, we were third among all the pihps in the state in terms of our score for the first year. So I'm excited about that. So I'm going to stop right there and entertain any questions that you may have. Oh, and one more thing I do want to mention that it's my hope in September that I can give you some data on our performance monitoring metrics, the quality teams right now as we, as I speak, is out there monitoring our system, and I'm hoping to bring some of that information back to You, hopefully in September, when we get all the information and analyze all the data and whatnot. Thank you. Thank Speaker 2
you. I'm very confident in your success. Also, are there any questions or comments? Okay, nope, okay, thank you. And we are on to clinical operations summary, thank
Speaker 8
you. Good afternoon again. Board members. Melissa moody, VP of Clinical Operations, I'm just going to highlight a few things out of my report. One is in relation to our autism services. I know Ms Phipps earlier today did the autism report. I just wanted to kind of add on to that, something that we really were looking into as we continue to see costs increase in the autism benefit that's been happening over the last few years, and we took a deeper dive to look into those costs, what we're really seeing is a really big increase in persons requesting and being approved for their services. We did a in depth analysis of the utilization of those services, what services are being provided, and when we look at that, we determine there is no, there's no over utilization going on. Actually, it's on the very conservative side of those services being provided. And just something to note, you know, we've seen a substantial increase in not only the treatment, but a really large increase in persons being evaluated for autism, which really is in line with what they're saying with the CDC in 2022 the CDC report across 16 different sites they were looking at, they said autism was one in 31 for eight year olds and one In 34 for four year olds, which is a 375% increase since the year 2000 so there's been a huge, huge increase in the autism rates over the years, and I think that's something we're going to have to be talking to MDHHS about and things like that when we Need to continue to support this program going forward. The other couple things I wanted to talk about. One, of course, is our certified community behavioral health clinic services for our provider 
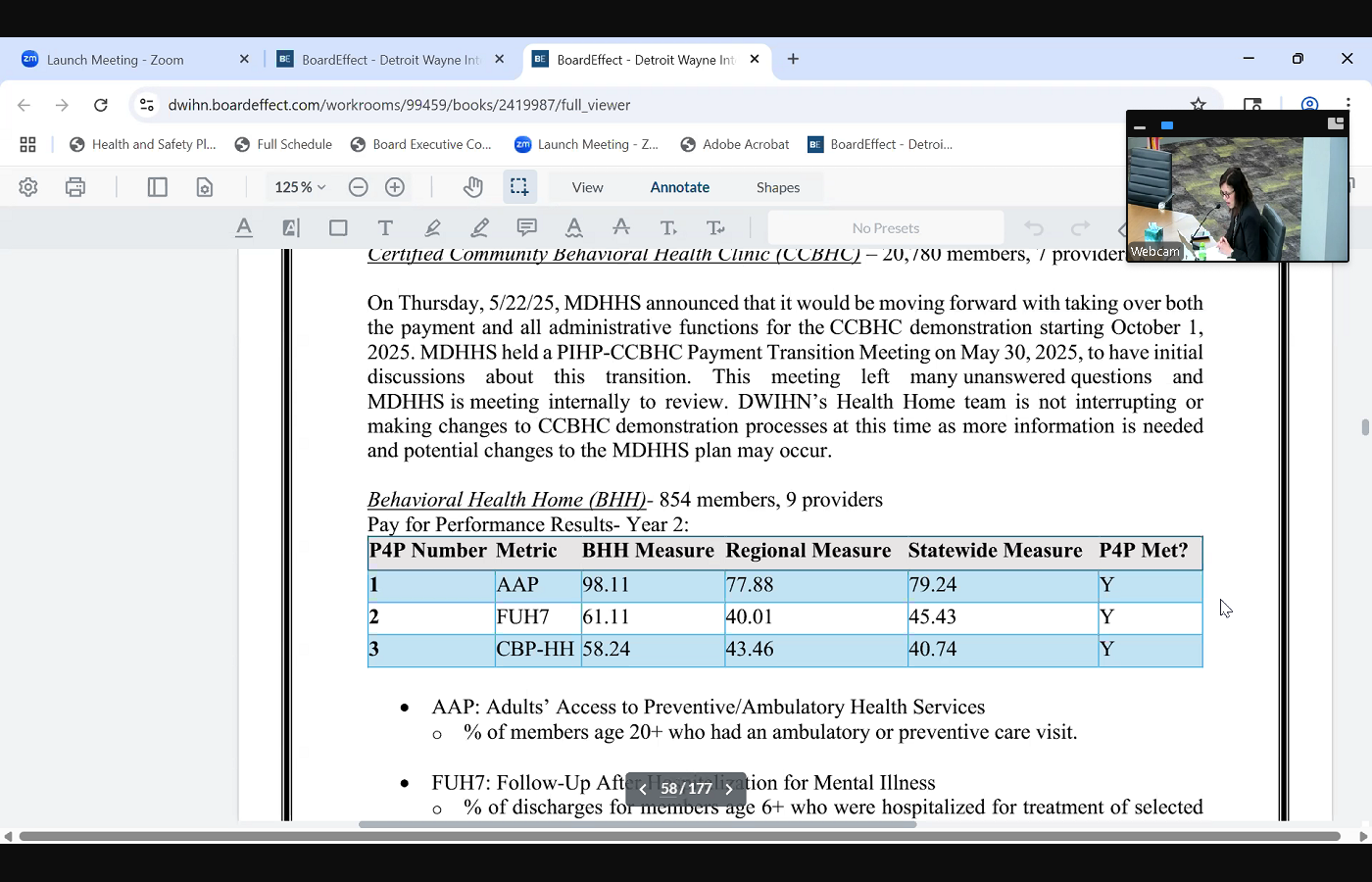 network currently have over 20,780 members across seven providers. We were recently told by MDHHS that starting in October, they would be doing direct payment for those services. Right now this the funds for ccbhcs come through Detroit, Wayne, but in the future, the state will be contracting with those providers directly moving forward. So we are having several meetings to discuss what that transition looks like as of October, one a couple other things, our behavioral health home last month, I talked about the success in that program, that we met our regional and statewide measures. I think the day after I reported on that we received our outcomes for our substance use, our substance use disorder, health homes and for year three performance results, we also met those performance members measures for year three, so we're going to be getting incentives based on those performance measures as well. Just wanted to highlight a couple of successes in our substance use disorder, health, home wellness challenge continues to have positive results. One of these challenges is for persons to go to a primary care provider and have screening labs completed. Through this initiative, new light identified two members that had undiagnosed hepatitis and several others had undiagnosed diabetes, and the screening allowed identification and enabled those members to start receiving the appropriate medical care for those physical issues. I think that's what I'm going to focus on for today. So have any questions for me?
network currently have over 20,780 members across seven providers. We were recently told by MDHHS that starting in October, they would be doing direct payment for those services. Right now this the funds for ccbhcs come through Detroit, Wayne, but in the future, the state will be contracting with those providers directly moving forward. So we are having several meetings to discuss what that transition looks like as of October, one a couple other things, our behavioral health home last month, I talked about the success in that program, that we met our regional and statewide measures. I think the day after I reported on that we received our outcomes for our substance use, our substance use disorder, health homes and for year three performance results, we also met those performance members measures for year three, so we're going to be getting incentives based on those performance measures as well. Just wanted to highlight a couple of successes in our substance use disorder, health, home wellness challenge continues to have positive results. One of these challenges is for persons to go to a primary care provider and have screening labs completed. Through this initiative, new light identified two members that had undiagnosed hepatitis and several others had undiagnosed diabetes, and the screening allowed identification and enabled those members to start receiving the appropriate medical care for those physical issues. I think that's what I'm going to focus on for today. So have any questions for me?
+3
network currently have over 20,780 members across seven providers. We were recently told by MDHHS that starting in October, they would be doing direct payment for those services. Right now this the funds for ccbhcs come through Detroit, Wayne, but in the future, the state will be contracting with those providers directly moving forward. So we are having several meetings to discuss what that transition looks like as of October, one a couple other things, our behavioral health home last month, I talked about the success in that program, that we met our regional and statewide measures. I think the day after I reported on that we received our outcomes for our substance use, our substance use disorder, health homes and for year three performance results, we also met those performance members measures for year three, so we're going to be getting incentives based on those performance measures as well. Just wanted to highlight a couple of successes in our substance use disorder, health, home wellness challenge continues to have positive results. One of these challenges is for persons to go to a primary care provider and have screening labs completed. Through this initiative, new light identified two members that had undiagnosed hepatitis and several others had undiagnosed diabetes, and the screening allowed identification and enabled those members to start receiving the appropriate medical care for those physical issues. I think that's what I'm going to focus on for today. So have any questions for me? 
Speaker 2
No, I have no questions. Did you have any questions? No, thank you. Thank you. We're moving on to unfinished business and their two board actions, autism service providers. You
Speaker 3
Good  afternoon again, hopefully this will be the last time at the podium. Cassandra Phipps, Director of children's initiatives, presenting board action, 25 dash, 24 r4 this is the fourth revision of adding additional ABA providers to the network, there will be three, blue mind therapy, bright behavior therapy, and the third one, there is a correction to this name. There's a typo. It's actually integrated pediatric therapy is the name. And so the total amount will not change for this contract, but it's to add the three new providers. I Yes,
afternoon again, hopefully this will be the last time at the podium. Cassandra Phipps, Director of children's initiatives, presenting board action, 25 dash, 24 r4 this is the fourth revision of adding additional ABA providers to the network, there will be three, blue mind therapy, bright behavior therapy, and the third one, there is a correction to this name. There's a typo. It's actually integrated pediatric therapy is the name. And so the total amount will not change for this contract, but it's to add the three new providers. I Yes,
+1
afternoon again, hopefully this will be the last time at the podium. Cassandra Phipps, Director of children's initiatives, presenting board action, 25 dash, 24 r4 this is the fourth revision of adding additional ABA providers to the network, there will be three, blue mind therapy, bright behavior therapy, and the third one, there is a correction to this name. There's a typo. It's actually integrated pediatric therapy is the name. And so the total amount will not change for this contract, but it's to add the three new providers. I Yes, Speaker 2
support all those in favor, say aye, aye. Abstentions, nays, thank you. Next. Board action provider, network systems, good
Speaker 16
afternoon.  Board members. Ray Williams, Director of contract management, here to present board action. 2551 revision four for our provider network systems. Board action, dwin is requesting the addition of three providers. Are all residential providers caring for others, home care solutions, Mimi LLC and real people cares LLC. There will be no change to the budget. Thank you.
Board members. Ray Williams, Director of contract management, here to present board action. 2551 revision four for our provider network systems. Board action, dwin is requesting the addition of three providers. Are all residential providers caring for others, home care solutions, Mimi LLC and real people cares LLC. There will be no change to the budget. Thank you.
+1
Board members. Ray Williams, Director of contract management, here to present board action. 2551 revision four for our provider network systems. Board action, dwin is requesting the addition of three providers. Are all residential providers caring for others, home care solutions, Mimi LLC and real people cares LLC. There will be no change to the budget. Thank you. Unknown Speaker
Move for approval.
Unknown Speaker
There's support.
Unknown Speaker
Any questions, discussion,
Speaker 2
all those in favor, please say Aye, Aye. Nays, abstentions, approved. Thank you. A new business board action, 64 HUD, permanent supporting housing.
Speaker 16
Apologies, 
 I have this one too, right. Ray Williams, again, Director of contract management, here to present board action. 2564 this is our HUD, permanent supportive housing board action. Dwin is requesting the approval to renew and disperse our US, Department of Housing and Urban Development, continuum of care, permanent supportive housing funds to the following providers, cots, which is the coalitions Development Center Central City, Southwest counseling solutions and Wayne Metro Community Action. Additionally, this board action recommends approval of disbursement of our local match to DCI cots and CCI H. Total amount for this board action is 2000 or No, excuse me. $2,773,935.50
I have this one too, right. Ray Williams, again, Director of contract management, here to present board action. 2564 this is our HUD, permanent supportive housing board action. Dwin is requesting the approval to renew and disperse our US, Department of Housing and Urban Development, continuum of care, permanent supportive housing funds to the following providers, cots, which is the coalitions Development Center Central City, Southwest counseling solutions and Wayne Metro Community Action. Additionally, this board action recommends approval of disbursement of our local match to DCI cots and CCI H. Total amount for this board action is 2000 or No, excuse me. $2,773,935.50
+2
I have this one too, right. Ray Williams, again, Director of contract management, here to present board action. 2564 this is our HUD, permanent supportive housing board action. Dwin is requesting the approval to renew and disperse our US, Department of Housing and Urban Development, continuum of care, permanent supportive housing funds to the following providers, cots, which is the coalitions Development Center Central City, Southwest counseling solutions and Wayne Metro Community Action. Additionally, this board action recommends approval of disbursement of our local match to DCI cots and CCI H. Total amount for this board action is 2000 or No, excuse me. $2,773,935.50 Unknown Speaker
Thank you. Is there a motion
Unknown Speaker
move for approval?
Unknown Speaker
Any questions discussion? Yes,
Speaker 16
correct. We are the recipient of these HUD grants, and these are the sub recipients.
Unknown Speaker
All those in favor, please say Aye.
Speaker 2
Nays,  abstentions, approved. Thank you. And do you have 65 No, okay, all right, our last board action, Western Wayne therapeutic Good
abstentions, approved. Thank you. And do you have 65 No, okay, all right, our last board action, Western Wayne therapeutic Good
+1
abstentions, approved. Thank you. And do you have 65 No, okay, all right, our last board action, Western Wayne therapeutic Good Speaker 17
afternoon. Andrea Smith, I am presenting board action 2565 which is requesting approval to enter into agreement with Canton township for the Western Wayne therapeutic recreation program for the amount of $75,000 this will the amount is 75,000 for the second year, based on them covering other communities in western Wayne County, outside of Canton. Thank you.
Unknown Speaker
There a motion
Unknown Speaker
move for approval.
Speaker 2
Support, support, questions, discussion. All those in favor, please say Aye. Any nays, abstentions, approved. Thank you. Thank you. And we are now at good and welfare. And before I make Yes, oh, I'm sorry, Madam Chair,
Speaker 11
if you don't mind, Mr. White is also with us remotely, because he's at the conference, and he would like to make a comment, oh,
Speaker 2
thank you, Mr. White, I'm sorry I did not acknowledge you before now and only at the beginning.
Speaker 18
No problem at all. Hopefully you can hear me. I'm having some trouble. Can you hear
Unknown Speaker
me? Okay, yes, we can,
Unknown Speaker
all right. Um, just a
Speaker 18
couple of things. I just wanted to commend everyone on the comprehensive presentations, it seems like to me that they get better each time I hear them. They were very conversational and brought a lot of really good information to everyone. I do agree. I think that a department overview from everyone would be beneficial, not only for the board, but for myself, so we're going to move in that direction. I think that's a great idea. The other issue that came up with regards to, I think, was Dr Carter, who asked about the outcome of the calls when people are waiting, or the the number of calls that we receive in the waiting period, I think, is just a few seconds. We've already started to look at those calls. Manny, in fact, is building out a process where we're going to audit the calls, just to make sure that we can best serve the people who call. The other issue that came up with regards to what do we call folks that call whether they're customers or or potential members, we'll look at that. I think potential members, but certainly people works as well. So those are only things I wanted to comment on, and sadly, I'm sure that it's probably making its way around, but Commissioner Clark Coleman has died, and I know that she's very close to DWIHN. I knew her personally, and a very sad day, I just wanted to put put that out there as well.
Speaker 2
Thank you for both the comments and acknowledgement of the recommendations and then the making us aware of the death of the commissioner. Yes, are there any other comments or questions
Speaker 4
as relates to the reports today, they were outstanding. And so whatever processes we're doing or in order to move them in that direction, just continue to do that, because everyone did a great job today. So applause to you guys. You did an excellent job.
Speaker 2
You speak for all of us, and thank you for saying it out loud. Trent, is there anyone on the phone?
Speaker 19
Good afternoon, Madam Chair, we do have guests with us today. The offer to make public comment has been extended via the chat. No one has raised their hand to make public comment. I don't believe there's anyone in the audience who would like to make comment. Did we receive any comment cards? No. So no public comment.
Speaker 2
Well, with that in mind, the meeting program compliance for June is adjourned. Thank you everybody very much.
Unknown Speaker
recording stopped.