Loading...
DWIHN, Program Compliance Committee
Speaker 1
recording in progress. Good afternoon, everyone. I like to call to order the meeting of the Detroit Wayne Integrated Health Network program Compliance Committee meeting. My name is Cynthia tag. I'm the chair of this group. We've got a full committee presence today and we've got a very full agenda. So we will go ahead and get started. So at this point, let's take just a moment of silence we can get ourselves all centered and focused on the business at hand.
Speaker 1
Thank you. I guess also, I just want to say just really feeling a special point of concern and compassion towards the folks in Morocco and Libya, where they're undergoing extreme extreme disaster, natural disasters and loss of life and grief. So, just wanted to acknowledge that all right, roll call vote, miss. A black shy would you do that words, please? Yes, Madam Chair.
Unknown Speaker
Dr. Tag present. Thank you. Mr. Phillips. Thank you, Miss Bullock President. Thank you, Dr. Carter. Thank you, Commissioner kilmallock. Present. Thank you, Mr. Parker. Thank you. Are there any board members that are joining the meeting via zoom? Are there any board members joining the meeting? Via zoom?
Unknown Speaker
Madam Chair, you do have a quorum. Thank
Speaker 1
you. Thank you. Thank you, everyone. As I look at our agenda again, we do have a very full agenda. So I do need a motion to approve the agenda as presented to us today will remove move by Mr. Parker support support by Mr. Bullock. Any further discussion on the agenda?
Speaker 2
Madam Chair? Yes, if I may. Yes, we needed to add board action 2417 to the agenda.
Speaker 1
Yes, I was aware and I overlooked that. Thank you for that reminder. So we are adding one additional board action to the agenda. What is that number again, please. Lillian.
Speaker 2
Madam Chair, it's born action 2417 And it is the school success Health Quality Initiative.
Speaker 1
Thank you. So please note that board members and with that addition, we do have a motion on the floor to approve the agenda any further discussion? The no hands all in favor signify by saying aye. Aye. Any opposed? Any abstentions? Thank you. Thank you. All right. We've got again quite a bit to cover quite a bit to cover so we'll just proceed on to the end. So the first item will be some follow up items. So corporate compliance is Jackson, do you want to take us through that information?
Speaker 3
Good afternoon, Madam Chair as a follow up per our previous discussion. corporate compliance will report out during program Compliance Committee quarterly but as additional things occur, such as things that are emergent things that are reported to the state of Michigan, I will then report out to this board.
Speaker 1
Thank you and there is a report in the meeting so I guess we'll get to it when we when we get to it yes, that is correct. I did ask about some criteria, but I think we can just kind of go with the flow and see how that goes. In terms of criteria for exceptional reporting that is reporting outside of the normal quarterly report or the newly established quarterly report. All right. Also Children's Services quarterly report, there was a follow up item. That's pips I believe.
Speaker 4
Good afternoon, everyone. Cassandra is director of children's initiatives. I'm actually presenting the quarterly report later on the agenda. If I could answer that response altogether, if that will please the board.
Speaker 1
Well, that will be fine with me. And that answer to our request, information is included. Correct.
Unknown Speaker
I can Yes, I can give a verbal response for that. Okay. Yes,
Speaker 1
we're good. All right. We can delay that till then. All right. Moving on then with our agenda. I need approval of the minutes from our July 12 meeting. Remember, there was no August meeting. So we'll have the minutes I need a motion please. Move by Mr. Parker is a support support by Dr. Carter. Any further discussion? The no hands all in favor signify by saying aye. Aye. Any opposed? Any abstentions? Thank you. All right. We've got some reports chief medical officer, Dr. Faheem. Please go ahead.
Speaker 5
Good  afternoon Madam Chair respected Board shall my Faheem chief medical officer degreed me. I'll start my report with some updates around the education and our outreach efforts. As we continue to outreach. The Ask the doc newsletter has continued and the last tradition in August focused on back to school stress, as well as some important children and vaccines that are required. During that time. We have been focusing on collaborating with teaching programs, particularly Wayne State University, not only to increase our awareness about the community mental health, but also to create pipeline programs for various disciplines. I'm scheduled for lectures on CME agency and managed services for psychiatry residents as well as child and adolescent psychiatry fellows over the next six months. We have met with their leadership in terms of talking about irritation of psychiatry residents and as well as fellows the child psychiatry fellows at our crisis centers they submitted a sample GME contracts once we are more close to opening, the crisis center will end we have a date we will just go back and complete the program. description of what type of trainings they receive. They're going to submit that to ACGME and that's when we would have a final approval of that. We also met with physician assistant school at Penn State in July. Their program director was also very much interested in rotation of PA students at the crisis center. They shared their general expectations from the rotations and again that would be finalized as soon as we have a confirmed opening date. We also met with Wayne State School of Social Work who are interested in rotation of their students and interns at the crisis center. The rotation runs from October through April. So we'll meet again in January to see if we can accommodate the current TAs that is going to end their kinda year in April and offer some rotations to them or just wait until October. 2024 to start that piece. The have also met Where do you have an adolescent child and adolescent service chiefs they reached out they wanted to know about all the services they get some complex behavioral health patients and they wanted to see how some of the services such as they were offered by us could augment some of their members. I shared all the resources and scheduled quarterly meeting. We're planning to address some of the UFM psychiatry residents and child psychiatry follows the chain and how community mental health service education could be incorporated in
afternoon Madam Chair respected Board shall my Faheem chief medical officer degreed me. I'll start my report with some updates around the education and our outreach efforts. As we continue to outreach. The Ask the doc newsletter has continued and the last tradition in August focused on back to school stress, as well as some important children and vaccines that are required. During that time. We have been focusing on collaborating with teaching programs, particularly Wayne State University, not only to increase our awareness about the community mental health, but also to create pipeline programs for various disciplines. I'm scheduled for lectures on CME agency and managed services for psychiatry residents as well as child and adolescent psychiatry fellows over the next six months. We have met with their leadership in terms of talking about irritation of psychiatry residents and as well as fellows the child psychiatry fellows at our crisis centers they submitted a sample GME contracts once we are more close to opening, the crisis center will end we have a date we will just go back and complete the program. description of what type of trainings they receive. They're going to submit that to ACGME and that's when we would have a final approval of that. We also met with physician assistant school at Penn State in July. Their program director was also very much interested in rotation of PA students at the crisis center. They shared their general expectations from the rotations and again that would be finalized as soon as we have a confirmed opening date. We also met with Wayne State School of Social Work who are interested in rotation of their students and interns at the crisis center. The rotation runs from October through April. So we'll meet again in January to see if we can accommodate the current TAs that is going to end their kinda year in April and offer some rotations to them or just wait until October. 2024 to start that piece. The have also met Where do you have an adolescent child and adolescent service chiefs they reached out they wanted to know about all the services they get some complex behavioral health patients and they wanted to see how some of the services such as they were offered by us could augment some of their members. I shared all the resources and scheduled quarterly meeting. We're planning to address some of the UFM psychiatry residents and child psychiatry follows the chain and how community mental health service education could be incorporated in
+1
afternoon Madam Chair respected Board shall my Faheem chief medical officer degreed me. I'll start my report with some updates around the education and our outreach efforts. As we continue to outreach. The Ask the doc newsletter has continued and the last tradition in August focused on back to school stress, as well as some important children and vaccines that are required. During that time. We have been focusing on collaborating with teaching programs, particularly Wayne State University, not only to increase our awareness about the community mental health, but also to create pipeline programs for various disciplines. I'm scheduled for lectures on CME agency and managed services for psychiatry residents as well as child and adolescent psychiatry fellows over the next six months. We have met with their leadership in terms of talking about irritation of psychiatry residents and as well as fellows the child psychiatry fellows at our crisis centers they submitted a sample GME contracts once we are more close to opening, the crisis center will end we have a date we will just go back and complete the program. description of what type of trainings they receive. They're going to submit that to ACGME and that's when we would have a final approval of that. We also met with physician assistant school at Penn State in July. Their program director was also very much interested in rotation of PA students at the crisis center. They shared their general expectations from the rotations and again that would be finalized as soon as we have a confirmed opening date. We also met with Wayne State School of Social Work who are interested in rotation of their students and interns at the crisis center. The rotation runs from October through April. So we'll meet again in January to see if we can accommodate the current TAs that is going to end their kinda year in April and offer some rotations to them or just wait until October. 2024 to start that piece. The have also met Where do you have an adolescent child and adolescent service chiefs they reached out they wanted to know about all the services they get some complex behavioral health patients and they wanted to see how some of the services such as they were offered by us could augment some of their members. I shared all the resources and scheduled quarterly meeting. We're planning to address some of the UFM psychiatry residents and child psychiatry follows the chain and how community mental health service education could be incorporated in Speaker 1
that video. I want to interrupt you for a second here. I noticed. I want to suggest that you reach out to the nursing school at Wayne State University. They have nurse practitioners, they also specialize in psychiatry, as well as nursing students go through a psychiatry rotation and also would like you to reach out to Wayne State has a public health program and mental health has so issues are so pervasive across all disciplines. I really didn't want to leave those two out. Of course I have a special affinity for both of those
Speaker 5
can be I think yeah, I've been I when we met with the the nurse practitioner program was I think it was more like the introduction that was we were connected to a lot of these through Dr. Close Holabird who is the and Dr. Milan on the adult psychiatry side, but definitely I'll reach out to the nurse practitioner and the nursing school myself. So that is on my to do list for sure.
Unknown Speaker
Thank you don't forget public health.
Unknown Speaker
No public health. Yes. I made a note.
Unknown Speaker
Thank you. You're going alright, objective. Yeah.
Speaker 5
I 
 also would, I'm delighted to talk about the next paragraph which is our new initiative. Highlight. We completed a grant on vigorous suicide back in May with the help of Andre Smith and our team. We were notified just a couple of days ago about being awarded 400,000 per year for launching the Event Zero Suicide initiative to eliminate suicides in Wayne County through system wide cultural change workforce training, comprehensive screening, evidence based treatment and care management. Our goal would be to launch Zero Suicide evidence based practices screening that directs em HSB functions such as crisis services clinics future forward as well as across network so that we are really excited about that it has a comprehensive plan in terms of how we are going to address the identification through training screening, strain the individuals and then provide some evidence based CBT suicide kind of practices. So we're really looking forward to that. We also submitted a proposal to MDHHS grant for my kids now mobile crisis services in May, and we were again notified them recently that we are approved for 200,000 grant pending permission of some revisions. And as of now, I think that is also taken care of so we are in into that grant as well. This grant would give us not only an opportunity to have child specific teams but one team to respond to the crisis in the community but also to be one of the cohort pilots that would be working with the state on standards and best practices. So definitely we want it to be on the table and we are excited that we would be on the table.
also would, I'm delighted to talk about the next paragraph which is our new initiative. Highlight. We completed a grant on vigorous suicide back in May with the help of Andre Smith and our team. We were notified just a couple of days ago about being awarded 400,000 per year for launching the Event Zero Suicide initiative to eliminate suicides in Wayne County through system wide cultural change workforce training, comprehensive screening, evidence based treatment and care management. Our goal would be to launch Zero Suicide evidence based practices screening that directs em HSB functions such as crisis services clinics future forward as well as across network so that we are really excited about that it has a comprehensive plan in terms of how we are going to address the identification through training screening, strain the individuals and then provide some evidence based CBT suicide kind of practices. So we're really looking forward to that. We also submitted a proposal to MDHHS grant for my kids now mobile crisis services in May, and we were again notified them recently that we are approved for 200,000 grant pending permission of some revisions. And as of now, I think that is also taken care of so we are in into that grant as well. This grant would give us not only an opportunity to have child specific teams but one team to respond to the crisis in the community but also to be one of the cohort pilots that would be working with the state on standards and best practices. So definitely we want it to be on the table and we are excited that we would be on the table.
+3
also would, I'm delighted to talk about the next paragraph which is our new initiative. Highlight. We completed a grant on vigorous suicide back in May with the help of Andre Smith and our team. We were notified just a couple of days ago about being awarded 400,000 per year for launching the Event Zero Suicide initiative to eliminate suicides in Wayne County through system wide cultural change workforce training, comprehensive screening, evidence based treatment and care management. Our goal would be to launch Zero Suicide evidence based practices screening that directs em HSB functions such as crisis services clinics future forward as well as across network so that we are really excited about that it has a comprehensive plan in terms of how we are going to address the identification through training screening, strain the individuals and then provide some evidence based CBT suicide kind of practices. So we're really looking forward to that. We also submitted a proposal to MDHHS grant for my kids now mobile crisis services in May, and we were again notified them recently that we are approved for 200,000 grant pending permission of some revisions. And as of now, I think that is also taken care of so we are in into that grant as well. This grant would give us not only an opportunity to have child specific teams but one team to respond to the crisis in the community but also to be one of the cohort pilots that would be working with the state on standards and best practices. So definitely we want it to be on the table and we are excited that we would be on the table. 
Speaker 6
Moving managers a quick taxpayer 400,000 for the suicide prevention that we determine whether it was 400,000 for the next five years.
Speaker 5
I somehow had a feeling you'll bring it up so yeah, so it is 400,000. If you read the grant, we initially thought that we are just receiving one time, but as we read the grant more, it's 400,000 per year for five years. And pending. Again they put all these caveats a little bit okay, pending submission, enough time he reports and Sam says availability of funding. So they might say okay, we don't have funding for the whole five years at some point, but if everything goes right then it is for five years. 400,000 per year, so super excited about that.
Speaker 1
Okay, great. Thanks for that clarification. That's great. Mr. Parker.
Speaker 7
has no way to DM but since you're getting some discussion now, are both of these grants internal that we're going to operate programs, or is it something that we're going to be contracting now?
Speaker 5
Both are going to be internal however, I would say that zero through the site would pan across we will have to make sure like you know that both internally and externally over Wayne County are rates are off to site are again so suicide is preventable. So they believe that Zero Suicide model believes that you can curb it down to zero. So that may require some programming or some sort of small project with the providers as well specifically looking at trends on where the suicide rates might be higher, but overall, this is an internal grant. Both are internal
Speaker 1
Okay, thank you. We'll be looking forward to updates as that be able to get us Bullock has a question for you. Yeah,
Speaker 5
go 
 ahead, please. Okay, no, can I use your microphone here? All right. So after all, that, I think the next topics where you will find this less interesting. I know there was a request about updating the board on some of the state hospital and their middle to Walter router and now that is going to be updated briefly based on the conversation I had but then we had a visit in July and August report was cancelled. So I've included that information. We visited Walter router back in July, after the children's side moved there. Houghton center is to be closed. It's not a hospital anymore. So basically Walter router has an adult wing and a child Bay. Dr. mallows and the hospital's leadership were there and they updated us on the processes incorporated to separate the adult and children wings, both physically and operationally. They talked about several critical spots where they have put in security to make sure that the only children or adults would be passing those points otherwise they're there. They augmented that with announcements and clearance that has to happen. They had very stringent scheduling that was put in place for common areas. Like library or do space and other areas that could be used by both groups so they cannot be used until reserve. They They did talk about a little downside to all of that where they felt like the adult population was using a lot of open space and now have to use it based on scheduling. So definitely that was a downside. They also mentioned about they had a hold on the children's admission for approximately two months and they told us that they are going to resume in September so we haven't heard a final word but it was
ahead, please. Okay, no, can I use your microphone here? All right. So after all, that, I think the next topics where you will find this less interesting. I know there was a request about updating the board on some of the state hospital and their middle to Walter router and now that is going to be updated briefly based on the conversation I had but then we had a visit in July and August report was cancelled. So I've included that information. We visited Walter router back in July, after the children's side moved there. Houghton center is to be closed. It's not a hospital anymore. So basically Walter router has an adult wing and a child Bay. Dr. mallows and the hospital's leadership were there and they updated us on the processes incorporated to separate the adult and children wings, both physically and operationally. They talked about several critical spots where they have put in security to make sure that the only children or adults would be passing those points otherwise they're there. They augmented that with announcements and clearance that has to happen. They had very stringent scheduling that was put in place for common areas. Like library or do space and other areas that could be used by both groups so they cannot be used until reserve. They They did talk about a little downside to all of that where they felt like the adult population was using a lot of open space and now have to use it based on scheduling. So definitely that was a downside. They also mentioned about they had a hold on the children's admission for approximately two months and they told us that they are going to resume in September so we haven't heard a final word but it was 
 to resume in September. I'm just wanted to quickly update. You know, the State Medical Director has monthly meetings with all PHP CMS recipes medical director to cover some important topics. I think the last time there was a robust discussion on the new Misha cans that would be launched. There. The program directors expressed some concerns about some of that. The most recent meeting that happened with the state medical directors. They also talked about how the state Sud gout guidelines kind of lag the federal guidelines and that creates a little bit of a confusion for our providers because they are looking through federal SAMSA guidelines, but then they're looking at the state guidelines that have not been updated for a couple of years. And they don't know which ones to follow. So I think that problem was both brought up to the stage and she said that she is going to address it with the Sud department and come back to us to give us an update. Also just wanted to let you know that I had our Chris medical directors meeting recently as well. A lot of them had questions about what is new in the
to resume in September. I'm just wanted to quickly update. You know, the State Medical Director has monthly meetings with all PHP CMS recipes medical director to cover some important topics. I think the last time there was a robust discussion on the new Misha cans that would be launched. There. The program directors expressed some concerns about some of that. The most recent meeting that happened with the state medical directors. They also talked about how the state Sud gout guidelines kind of lag the federal guidelines and that creates a little bit of a confusion for our providers because they are looking through federal SAMSA guidelines, but then they're looking at the state guidelines that have not been updated for a couple of years. And they don't know which ones to follow. So I think that problem was both brought up to the stage and she said that she is going to address it with the Sud department and come back to us to give us an update. Also just wanted to let you know that I had our Chris medical directors meeting recently as well. A lot of them had questions about what is new in the  crisis area. In terms of models. We invited our VP of crisis Grace walls to the last meeting she shared about the new evidence and the crisis area. There is a very robust discussion. Everybody really enjoyed what they learned from that meeting. And other topic that they brought up during that meeting was medication assisted treatment for individuals who had dual diagnosis. And that's where we have invited Judy Davis to our next meeting to address some of their questions around billing for the services and how that can be achieved. And last only just wanted to touch a little bit about the two important meetings that we do, which is improving in practice leadership team committee that talks about some of the new evidence that are coming around how we incorporated what the process is. And then we have representations from our providers to talk about the new guidelines and how we want to update it most recently we had a discussion about the last meeting we had the discussion about the discharge procedures and how we want to capture some of the discharge information and the reason for case closures. We also had a robust discussion about autism services and there were common shares that were you know for diagnosis it received through school, what would be some of the entry points that could skip the screening requirements. We are definitely exploring all of that feedback. We talked about a new guidelines around eating disorder that were reviewed and voted and agreed on. So those are some of the updates around IPL T and lastly quality improvement steering committee reviewed our actual survey come up, which was a survey that is given to our members for their feedback and basically a project plan was completed to make sure that all the items were the score was less than 60% were assigned to Leeds in those areas and a minimum of 10% improvement was identified. We are waiting to come back to the KYC for some updates in terms of achievement and the timeline. So that is the next goal but we we are moving forward with the plan off addressing that survey yearly and bringing it to Qi SC four to incorporate the feedback that we received from our members to come up with systemic changes that could address those things. That is the end of my report. Any questions?
crisis area. In terms of models. We invited our VP of crisis Grace walls to the last meeting she shared about the new evidence and the crisis area. There is a very robust discussion. Everybody really enjoyed what they learned from that meeting. And other topic that they brought up during that meeting was medication assisted treatment for individuals who had dual diagnosis. And that's where we have invited Judy Davis to our next meeting to address some of their questions around billing for the services and how that can be achieved. And last only just wanted to touch a little bit about the two important meetings that we do, which is improving in practice leadership team committee that talks about some of the new evidence that are coming around how we incorporated what the process is. And then we have representations from our providers to talk about the new guidelines and how we want to update it most recently we had a discussion about the last meeting we had the discussion about the discharge procedures and how we want to capture some of the discharge information and the reason for case closures. We also had a robust discussion about autism services and there were common shares that were you know for diagnosis it received through school, what would be some of the entry points that could skip the screening requirements. We are definitely exploring all of that feedback. We talked about a new guidelines around eating disorder that were reviewed and voted and agreed on. So those are some of the updates around IPL T and lastly quality improvement steering committee reviewed our actual survey come up, which was a survey that is given to our members for their feedback and basically a project plan was completed to make sure that all the items were the score was less than 60% were assigned to Leeds in those areas and a minimum of 10% improvement was identified. We are waiting to come back to the KYC for some updates in terms of achievement and the timeline. So that is the next goal but we we are moving forward with the plan off addressing that survey yearly and bringing it to Qi SC four to incorporate the feedback that we received from our members to come up with systemic changes that could address those things. That is the end of my report. Any questions?
+2
ahead, please. Okay, no, can I use your microphone here? All right. So after all, that, I think the next topics where you will find this less interesting. I know there was a request about updating the board on some of the state hospital and their middle to Walter router and now that is going to be updated briefly based on the conversation I had but then we had a visit in July and August report was cancelled. So I've included that information. We visited Walter router back in July, after the children's side moved there. Houghton center is to be closed. It's not a hospital anymore. So basically Walter router has an adult wing and a child Bay. Dr. mallows and the hospital's leadership were there and they updated us on the processes incorporated to separate the adult and children wings, both physically and operationally. They talked about several critical spots where they have put in security to make sure that the only children or adults would be passing those points otherwise they're there. They augmented that with announcements and clearance that has to happen. They had very stringent scheduling that was put in place for common areas. Like library or do space and other areas that could be used by both groups so they cannot be used until reserve. They They did talk about a little downside to all of that where they felt like the adult population was using a lot of open space and now have to use it based on scheduling. So definitely that was a downside. They also mentioned about they had a hold on the children's admission for approximately two months and they told us that they are going to resume in September so we haven't heard a final word but it was +2
to resume in September. I'm just wanted to quickly update. You know, the State Medical Director has monthly meetings with all PHP CMS recipes medical director to cover some important topics. I think the last time there was a robust discussion on the new Misha cans that would be launched. There. The program directors expressed some concerns about some of that. The most recent meeting that happened with the state medical directors. They also talked about how the state Sud gout guidelines kind of lag the federal guidelines and that creates a little bit of a confusion for our providers because they are looking through federal SAMSA guidelines, but then they're looking at the state guidelines that have not been updated for a couple of years. And they don't know which ones to follow. So I think that problem was both brought up to the stage and she said that she is going to address it with the Sud department and come back to us to give us an update. Also just wanted to let you know that I had our Chris medical directors meeting recently as well. A lot of them had questions about what is new in the +1
crisis area. In terms of models. We invited our VP of crisis Grace walls to the last meeting she shared about the new evidence and the crisis area. There is a very robust discussion. Everybody really enjoyed what they learned from that meeting. And other topic that they brought up during that meeting was medication assisted treatment for individuals who had dual diagnosis. And that's where we have invited Judy Davis to our next meeting to address some of their questions around billing for the services and how that can be achieved. And last only just wanted to touch a little bit about the two important meetings that we do, which is improving in practice leadership team committee that talks about some of the new evidence that are coming around how we incorporated what the process is. And then we have representations from our providers to talk about the new guidelines and how we want to update it most recently we had a discussion about the last meeting we had the discussion about the discharge procedures and how we want to capture some of the discharge information and the reason for case closures. We also had a robust discussion about autism services and there were common shares that were you know for diagnosis it received through school, what would be some of the entry points that could skip the screening requirements. We are definitely exploring all of that feedback. We talked about a new guidelines around eating disorder that were reviewed and voted and agreed on. So those are some of the updates around IPL T and lastly quality improvement steering committee reviewed our actual survey come up, which was a survey that is given to our members for their feedback and basically a project plan was completed to make sure that all the items were the score was less than 60% were assigned to Leeds in those areas and a minimum of 10% improvement was identified. We are waiting to come back to the KYC for some updates in terms of achievement and the timeline. So that is the next goal but we we are moving forward with the plan off addressing that survey yearly and bringing it to Qi SC four to incorporate the feedback that we received from our members to come up with systemic changes that could address those things. That is the end of my report. Any questions? Speaker 1
Are there any additional questions for Dr. Thinking? Just for my point of clarification, I didn't hear who the 400,000 Does the Zero Suicide Grant was the source of the grant SAMSA SAMSA.
Unknown Speaker
Grant and the other one is the MDHHS grant. Okay. All right. Thank you all right, seeing
Speaker 1
no further questions for you. Thank you. We will receive and file your report. All right, Miss Jackson, you're on corporate compliance.
Speaker 3
Okay, good afternoon distinguish for for third quarter, April one through June 30 2023. The Office of Inspector General report eight or excuse me referred a total of nine cases to our department for review. i This is actually a decrease from last quarter second quarter there were 12 total. I did a little investigating and collaborating with the Office of Inspector General to determine why these cases keep coming because they're older cases on while I was at buys the bus that five of the cases that reported during this quarter were from 2020. Dewayne conducted the investigations but we did not recoup the funds. So I was tasked with recouping the funds for those investigations that were conducted. I was advised that To date, there are no outstanding cases they have all been completed. So moving forward we should only receive up to date referrals that are coming in. We did it was total of $1,634 In addition, we had a data provider data breach on July 3 2023. We were notified by Central City Health about unauthorized access involving two of their employees they had in a threat actor access their emails within their emails. There was member information, though Central City Health reported 1414 members were access. There were total of 1364 members that were active with Dewayne currently, the information that was the access and close their full names, date of service, diagnostic scores, primary care physicians and treatment recommendations. I would like to know there are no social security numbers were affected nor financial information was assessed. I have met with our customer service department as well as our access Department provided them with information if we do receive any additional calls. Central City Health has been working with our members but they have sent out notification advising them of credit monitoring that's available to them. In addition to that upon stakeholder approval they'll be getting their high tech certification to ensure this doesn't happen moving forward.
Unknown Speaker
Yep, let's go look has a question for you. And then that's Carmen.
Speaker 8
Thank you, Madam Chair. Regarding the provider data breach, is the provider required to demonstrate what preventive measures that they have put in place to ensure this doesn't happen again, or have you seen anything? Yes,
Speaker 3
they have had they hired an outside cybersecurity company to come in and they revamped all of their policies. In addition to that they put firewalls up. So just as the windows they have that multifile factor authentication process that you have to use when accessing your email from external source. Thank you.
Speaker 9
Okay, that's what am I can you hear me? I can, what percentage of the 1364 does that represent of their entire population?
Speaker 3
I'm sorry for clarification. Are you asking for a B wins entire population or Central City Central City? That information I do not have to date but I can provide that so you
Speaker 9
just want to know is this a major breach or a minor breach?
Unknown Speaker
Okay, I will verify that for you and provide that to you.
Speaker 1
So that's the follow up item for the committee that mentioned sinners. Thank you. Yes, Mr. Parker.
Speaker 7
I'm not sure where or if there is even a investigation or complaint. I know that neighborhood service organization has reached out to me with a concern about a determination that the wind did or the state that gave them liability for situations that took place in the wider places. Is there any ongoing work or investigations being done? Around that or formal request from NSO?
Unknown Speaker
Madam Chair,
Unknown Speaker
just a minute who you're directing your question to miss.
Unknown Speaker
Yeah, Miss Jesse Jackson.
Speaker 1
Okay. Mr. Kellogg, let Commissioner respond and then I'll follow up. Okay. Miss Jackson.
Speaker 3
Okay, I'm sorry. Can you please rephrase your question? I guess is
Speaker 7
there any formal complaint or appeal from the neighborhood service organization, about a determination of their liability in a situation that took place at wonderful residential places?
Unknown Speaker
The compliance department has not received a form of appeal
Unknown Speaker
was the goal is there anything that is formally under consideration? By neighborhood service organization
Speaker 1
No. Thank you, Mr. Commissioner, Camelot.
Speaker 10
Yes, I just want to state that this organization that organization has consistently reached out to board members regarding an apparent incident that occurred at their organization. And I think that it is it's been said but not publicly stated. But since this is the first time it actually came forward, but it's inappropriate for them to be reaching out to board members, when there is not an investigation as it relates to Dean when but they absolutely understand who the point of contact is that who they should be contacting. And I think that it's inappropriate for them to continue to be reaching out to members of this board, as it relates to an outstanding our ongoing review by the state of Michigan. Regarding an incident that occurred at their facility. I just want to state that for the record.
Speaker 1
I'm aware of that Miss situation and it's a recipient, right. So there's a whole set of rules around the city and right so that's why it does not anything like that Mr. Parker has not shown up in our complaint, corporate compliance issue. But Miss Jackson were you going to make another comment?
Speaker 3
I would. I would just like to note that this is a legal matter. This was this situation has been referred to our legal department. So I do ask that if the board has questions pertaining to this, that you do address it with the legal department on the record.
Speaker 1
Mr. Doe, did you want to make a comment on this issue?
Unknown Speaker
No, ma'am. I have Okay, comments. All right.
Unknown Speaker
Okay, Mr. Parker, so
Speaker 7
I understand now is in a legal department. I didn't know where was that.
Unknown Speaker
Okay, all right. Miss Jackson. Continue with your report, please.
Speaker 11
Okay, question. Okay. So, what this looks like is a potential violation. Do we have any exposure we do not. And as it relates, I know from being in the state, they have increased their cybersecurity requirements. There are certain things that they are now required that all vendors have and that they have in place. And we take it any step similar to that which this is the US. Of course we've been we taken any steps similar to the state that are required by others to have similar protections and policies. In place for cybersecurity purposes. We grabbed
Speaker 12
many signals to pick up so just wanted to state that in lieu of some there was a similar case that happened with one of our providers earlier. We went out and reached out to the network to ensure everybody is complying for this contract here. A high trust certification, which is going to enforce both from a policy standpoint, or a procedure standpoint, whether you talk about a multi factor authentication, whether you talk about introducing education resources within the workforce, as an expectation, but there has not been enforcement to answer your question directly. That is something we're looking to do as more of these cases and from a compliance standpoint where they stand.
Speaker 11
I would suggest that we take a look at their vendors and then it takes similar actions because being married to a cybersecurity expert, I hear every day that these way are these these the thieves to get into your systems to your vision and they look for weak weak spots within your vendor. So I would suggest that we grab a hold of that. Absolutely have those policies now. That's a good point.
Speaker 1
All right. Thank you. Miss Jackson, you want to continue your report, please.
Speaker 3
Yes, that actually concludes my report, but I would like to follow up to Dr. Carter's question, just so that everyone is aware of Central City Health has a total of 6580 D when members of that 1414 members they reported were effective. But again, I stated that once we looked into our system, there were a total of 1364 members that were actually affected,
Speaker 1
if that's it when members I think Dr. Carter, correct me if I'm wrong. Dr. Carter, you asked you about the total Central City's population, correct.
Unknown Speaker
Okay. I will verify that question. I'm sorry.
Unknown Speaker
Central City to all of the members. We did not send out anything because, okay.
Unknown Speaker
All right. That concludes your report on Miss Jackson.
Unknown Speaker
It does Madam Chair. All right.
Speaker 1
Any 
 further questions for Miss Jackson? All right. Thank you, Miss Jackson. We will receive and file your report. Then we'll move on right along then with our agenda. Our next we look at now some quarterly reports. I would ask that with the quarterly reports. You've got a number of them that you all please focus on the highlights. I know there's a lot of good detail in some of them. So if it's something new or something significant, you know, focus on that. Some of the detail. We might not need to go over verbally. All right. Let's start then. Well, of course with the access call center
further questions for Miss Jackson? All right. Thank you, Miss Jackson. We will receive and file your report. Then we'll move on right along then with our agenda. Our next we look at now some quarterly reports. I would ask that with the quarterly reports. You've got a number of them that you all please focus on the highlights. I know there's a lot of good detail in some of them. So if it's something new or something significant, you know, focus on that. Some of the detail. We might not need to go over verbally. All right. Let's start then. Well, of course with the access call center
+2
further questions for Miss Jackson? All right. Thank you, Miss Jackson. We will receive and file your report. Then we'll move on right along then with our agenda. Our next we look at now some quarterly reports. I would ask that with the quarterly reports. You've got a number of them that you all please focus on the highlights. I know there's a lot of good detail in some of them. So if it's something new or something significant, you know, focus on that. Some of the detail. We might not need to go over verbally. All right. Let's start then. Well, of course with the access call center Speaker 13
Good afternoon, everyone. Afternoon. For the access call center for the third quarter. You can say your name, please. I'm sorry. My name is Yvonne Bostick. I'm the director of Darwin's access cost center.
Unknown Speaker
It's not for me, it's for the listeners.
Speaker 13
I  apologize. Okay, thanks. For the third quarter fiscal year 20 to 23. There were a total of 54,256 Incoming Calls. That was a decrease from the second quarter by 315 calls. When we did an annual comparison from fiscal year 2122 to fiscal year 20 to 23. We received 12,000 more calls this year than we did last year. This quarter. We did meet our state standards. For our abandonment percentage goal is to be less than 5% and we were at 3.4% this quarter. The average speed to answer call should be less than 30 seconds we were at 28 seconds this quarter percentage of calls answered should be 80% or more. We were at 96.5%. And our service level goal is to be more than 80%. We were at 81 Point 83% for this quarter. Thank you. We continue to do assessments and things to see what we can do to improve these goals and improve our performance to meet these goals. We have continued training, coaching and we've made changes to our silent monitoring systems so that we can better analyze the calls and see where our trouble areas are to troubleshoot and see how we can
apologize. Okay, thanks. For the third quarter fiscal year 20 to 23. There were a total of 54,256 Incoming Calls. That was a decrease from the second quarter by 315 calls. When we did an annual comparison from fiscal year 2122 to fiscal year 20 to 23. We received 12,000 more calls this year than we did last year. This quarter. We did meet our state standards. For our abandonment percentage goal is to be less than 5% and we were at 3.4% this quarter. The average speed to answer call should be less than 30 seconds we were at 28 seconds this quarter percentage of calls answered should be 80% or more. We were at 96.5%. And our service level goal is to be more than 80%. We were at 81 Point 83% for this quarter. Thank you. We continue to do assessments and things to see what we can do to improve these goals and improve our performance to meet these goals. We have continued training, coaching and we've made changes to our silent monitoring systems so that we can better analyze the calls and see where our trouble areas are to troubleshoot and see how we can 
 streamline things so that we can have better performance and answer more calls. We recently added an addition to our script to inform callers that our wait times may be a little more during certain times and give them more options. To have a follow up call back later or if they want to wait on hold. We've we're working to make additions to our hold queue so that they can inform the person of like where they are in position. And if they decide not to hold any more than they can have that option to have their call returned to later during third quarter, we fill vacancies for our access call center quality improvement manager and our excess call center clinical manager and we hired two part time call center clinicians and one part time Sud tech. In this fourth quarter going we have also filled some of our vacancies for our clinical and Sud with part time and full time positions. And we are working on recruiting and hiring more staff so that we can better meet our call volumes. Looking at our silent monitoring we completed silent monitoring of 373 calls this quarter. The average was 91.3%. Overall, the goal is 95%. And again we are looking at ways that we can troubleshoot and work with our staff so that we can get closer to that goal. weak points this quarter included informing callers about the free translation services are three factor verification and completing screenings in a timely manner. To address those weaknesses. We are having additional trainings and our monthly staff meetings and during one on one supervision if we've identified individuals who are below the mark, they are getting additional coaching and reminders to make sure that they do these things so they
streamline things so that we can have better performance and answer more calls. We recently added an addition to our script to inform callers that our wait times may be a little more during certain times and give them more options. To have a follow up call back later or if they want to wait on hold. We've we're working to make additions to our hold queue so that they can inform the person of like where they are in position. And if they decide not to hold any more than they can have that option to have their call returned to later during third quarter, we fill vacancies for our access call center quality improvement manager and our excess call center clinical manager and we hired two part time call center clinicians and one part time Sud tech. In this fourth quarter going we have also filled some of our vacancies for our clinical and Sud with part time and full time positions. And we are working on recruiting and hiring more staff so that we can better meet our call volumes. Looking at our silent monitoring we completed silent monitoring of 373 calls this quarter. The average was 91.3%. Overall, the goal is 95%. And again we are looking at ways that we can troubleshoot and work with our staff so that we can get closer to that goal. weak points this quarter included informing callers about the free translation services are three factor verification and completing screenings in a timely manner. To address those weaknesses. We are having additional trainings and our monthly staff meetings and during one on one supervision if we've identified individuals who are below the mark, they are getting additional coaching and reminders to make sure that they do these things so they  can meet those goals. The updates that have been made to our silent monitoring process. They are to help us meet the requirements for our H sag and Ico and NCQA standards. So those changes that were made this quarter and moving forward. We are going to address those in our policies and procedures as well. Our areas of concern for third quarter there were 3215 appointments scheduled and of those 391 were scheduled outside of the 14th day. So that brought us to a 12% non compliance for our SCD, smi and DD appointments. We are meeting regularly with providers and we do contact providers regularly to see if we can get appointments added to the calendar so that we can meet that 14 day requirement. A lot of the providers have mentioned that they're still having difficulty with staffing. So that could be a large reason why we're having that difficulty. Plans for 2322 23/4 quarter for
can meet those goals. The updates that have been made to our silent monitoring process. They are to help us meet the requirements for our H sag and Ico and NCQA standards. So those changes that were made this quarter and moving forward. We are going to address those in our policies and procedures as well. Our areas of concern for third quarter there were 3215 appointments scheduled and of those 391 were scheduled outside of the 14th day. So that brought us to a 12% non compliance for our SCD, smi and DD appointments. We are meeting regularly with providers and we do contact providers regularly to see if we can get appointments added to the calendar so that we can meet that 14 day requirement. A lot of the providers have mentioned that they're still having difficulty with staffing. So that could be a large reason why we're having that difficulty. Plans for 2322 23/4 quarter for
+1
apologize. Okay, thanks. For the third quarter fiscal year 20 to 23. There were a total of 54,256 Incoming Calls. That was a decrease from the second quarter by 315 calls. When we did an annual comparison from fiscal year 2122 to fiscal year 20 to 23. We received 12,000 more calls this year than we did last year. This quarter. We did meet our state standards. For our abandonment percentage goal is to be less than 5% and we were at 3.4% this quarter. The average speed to answer call should be less than 30 seconds we were at 28 seconds this quarter percentage of calls answered should be 80% or more. We were at 96.5%. And our service level goal is to be more than 80%. We were at 81 Point 83% for this quarter. Thank you. We continue to do assessments and things to see what we can do to improve these goals and improve our performance to meet these goals. We have continued training, coaching and we've made changes to our silent monitoring systems so that we can better analyze the calls and see where our trouble areas are to troubleshoot and see how we can +2
streamline things so that we can have better performance and answer more calls. We recently added an addition to our script to inform callers that our wait times may be a little more during certain times and give them more options. To have a follow up call back later or if they want to wait on hold. We've we're working to make additions to our hold queue so that they can inform the person of like where they are in position. And if they decide not to hold any more than they can have that option to have their call returned to later during third quarter, we fill vacancies for our access call center quality improvement manager and our excess call center clinical manager and we hired two part time call center clinicians and one part time Sud tech. In this fourth quarter going we have also filled some of our vacancies for our clinical and Sud with part time and full time positions. And we are working on recruiting and hiring more staff so that we can better meet our call volumes. Looking at our silent monitoring we completed silent monitoring of 373 calls this quarter. The average was 91.3%. Overall, the goal is 95%. And again we are looking at ways that we can troubleshoot and work with our staff so that we can get closer to that goal. weak points this quarter included informing callers about the free translation services are three factor verification and completing screenings in a timely manner. To address those weaknesses. We are having additional trainings and our monthly staff meetings and during one on one supervision if we've identified individuals who are below the mark, they are getting additional coaching and reminders to make sure that they do these things so they +1
can meet those goals. The updates that have been made to our silent monitoring process. They are to help us meet the requirements for our H sag and Ico and NCQA standards. So those changes that were made this quarter and moving forward. We are going to address those in our policies and procedures as well. Our areas of concern for third quarter there were 3215 appointments scheduled and of those 391 were scheduled outside of the 14th day. So that brought us to a 12% non compliance for our SCD, smi and DD appointments. We are meeting regularly with providers and we do contact providers regularly to see if we can get appointments added to the calendar so that we can meet that 14 day requirement. A lot of the providers have mentioned that they're still having difficulty with staffing. So that could be a large reason why we're having that difficulty. Plans for 2322 23/4 quarter for Speaker 1
a moment just this Bullock has a question for you. On that point.
Speaker 8
Given our performance at 12%. Can you clarify what the standard we're aiming towards is? Well,
Speaker 13
I mean, ultimately we'd like to have zero in that area. We don't want to schedule people outside of the 14 days. It increases the likelihood of them no showing or missing appointments.
Speaker 8
I guess I'm trying to determine what the threshold is for it to be defined as an area of concern.
Speaker 13
Okay. Well, I guess the 12% is the 12% out of the 3215 point screenings that we completed. We want to we wanted to schedule everyone on time. So I guess that just said 12%. We're not supposed to be scheduling people outside of the 14 days. If it's at all avoidable
Unknown Speaker
it sounds like a low number. So
Speaker 14
yeah. Thank you. April CBRE, Director of Quality Improvement. Our benchmark, the state just recently identified a benchmark for us with two a two way has to do with ensuring that members receive their bio psychosocial within 14 days. And our benchmark now is that fit well it will be effective first quarter, which will be fiscal year 2024 In January will be 57% for us, so we have to ensure that 50% 57% of our members are getting their bio psychosocial within 14 days. Obviously, our goal is to ensure that all of our members who seek services are receiving their bio psychosocial what the state has said our benchmark at 57% and is based on our data is based on the state based it on our data our performance within the last year, the last two years and so that's where we fall in that percentile of 57% Hope I answer your question
Speaker 8
you did. So if 57% have to be scheduled within 14 days then 43% can be out of compliance, which seems
Speaker 14
in right and that that is the benchmark that the state has set for us. But obviously our goal is a lot higher. I mean, obviously we want to ensure that all of our members who are accessing our access department, who's requesting services are getting that service within 14 days. But because this is a new standard that was pushed out by the state two years ago, and what they did, they were tracking the data of all the PHPs within the state to see how we were performing in getting members and they indicated that we fall meaning D when fall within that percentile of 57%. Again, that's not our goal. Although that's the state benchmark. Our goal is to ensure that anyone that accesses department access for service received their bio psychosocial within the 14 days.
Speaker 1
Thank you. Is it your good, Philip, you're good. Okay. Please continue as fast as I can. Thank you.
Speaker 13
Thank you moving forward into the fourth quarter, the access cost center. We are working to develop a new phone system. Currently we're in the design phases of that phone system and we're looking forward to training staff and with hopes of implementing it either before the New Year or the end of this year. Okay.
Unknown Speaker
Thank you. That concludes your report. Yes. All right, any questions further from his Bostick? Go ahead Mr. Phillips,
Speaker 11
or  we'll say this awesome other than the answer, oh, are very ambitious. is all on it. All the excellent. Can't be the point of the business credibly. Looking at the numbers
we'll say this awesome other than the answer, oh, are very ambitious. is all on it. All the excellent. Can't be the point of the business credibly. Looking at the numbers
+1
we'll say this awesome other than the answer, oh, are very ambitious. is all on it. All the excellent. Can't be the point of the business credibly. Looking at the numbers Speaker 1
this just single I do have a related question. I think it's been about a year ago, maybe a little less. You spoke about we had some issues with a call center you move people back in house and modify the staffing pattern. Do you think that's had a positive impact on his numbers we're hearing about today?
Speaker 12
Absolutely. I think that was a very good strategic move well supported. It took a while to get folks on the board but because especially for folks who were having technical challenges, were not able to have the right support, you know when they need one. That was it took a period of three months, four months working closely with identifying people who are struggling. And at the end of the day, everybody bought into it and now it's actually a very welcome change with people coming in. So it was very adequately supported even by the staff
Speaker 1
right. Thank you. Thank you. Definitely, I'm sure what.
Unknown Speaker
Even though it's not bad, but the next year today, your reasonable price.
Speaker 1
I really love your enthusiasm. I'm going to ask you that make sure you kind of kind of work with us on Mr. Parker.
Speaker 7
Yes, of course. I know. years back there was a concern about the the credentials of the people that are in the call center. If I recall, they had to have a master's degree in social work. Is that still the case though?
Speaker 13
So we have three different units of a call center or Access Center for reps our frontline. They don't have to have a master's degree but they are trained to like triage the calls. Then those calls go to our clinical and Sud technicians and specialists that they have master's levels or their license state license with them. l LM SW LPC LLP and then our substance DSRC ADC see ADC or they're on a development plan to achieve those lines. The alphabet LMNOP
Speaker 7
Are you having a challenge trying to get people in those positions because of that requirement?
Speaker 13
Occasionally? Yeah, that does make a barrier we do have individuals who may not have their full license but they've had a lot of experience. So we are looking at that to see if we can find like a middle ground where maybe they've had a lot of experience. They're able to perform these things but you know we also have to look at what MDHHS says.
Unknown Speaker
Thank you Madam Chair.
Speaker 1
Okay, thank you will receive and file your report and will Mr. Doe you have to watch Mr. Phillips So
Speaker 6
yes, and one question if you don't mind. As fast as you talk about those calls, waiting in the recording that comes on? I'm of course concern about those crisis calls. Are those different? Is there a difference between those calls that are coming in or, you know, crisis related matters?
Speaker 13
At the entry of the car when it gets to our Access Center? Rep. That's one of the first questions we ask is this a crisis call? Sometimes we have to ask a few additional questions to see what type of situation the person's in and if they need immediate attention. They're transferred to protocol for crisis calls, or they're given to one of our Access Center clinicians to engage 911 If we need to or what we need to do to make sure that person is safe.
Speaker 1
Thank you Thank you. Thank you. Thank you Miss Boston. All right. Well, now move on to the report from the Children's initiatives. I think that's misfits but yeah, here she comes.
Unknown Speaker
He's been our TV star we've seen
Speaker 4
Good 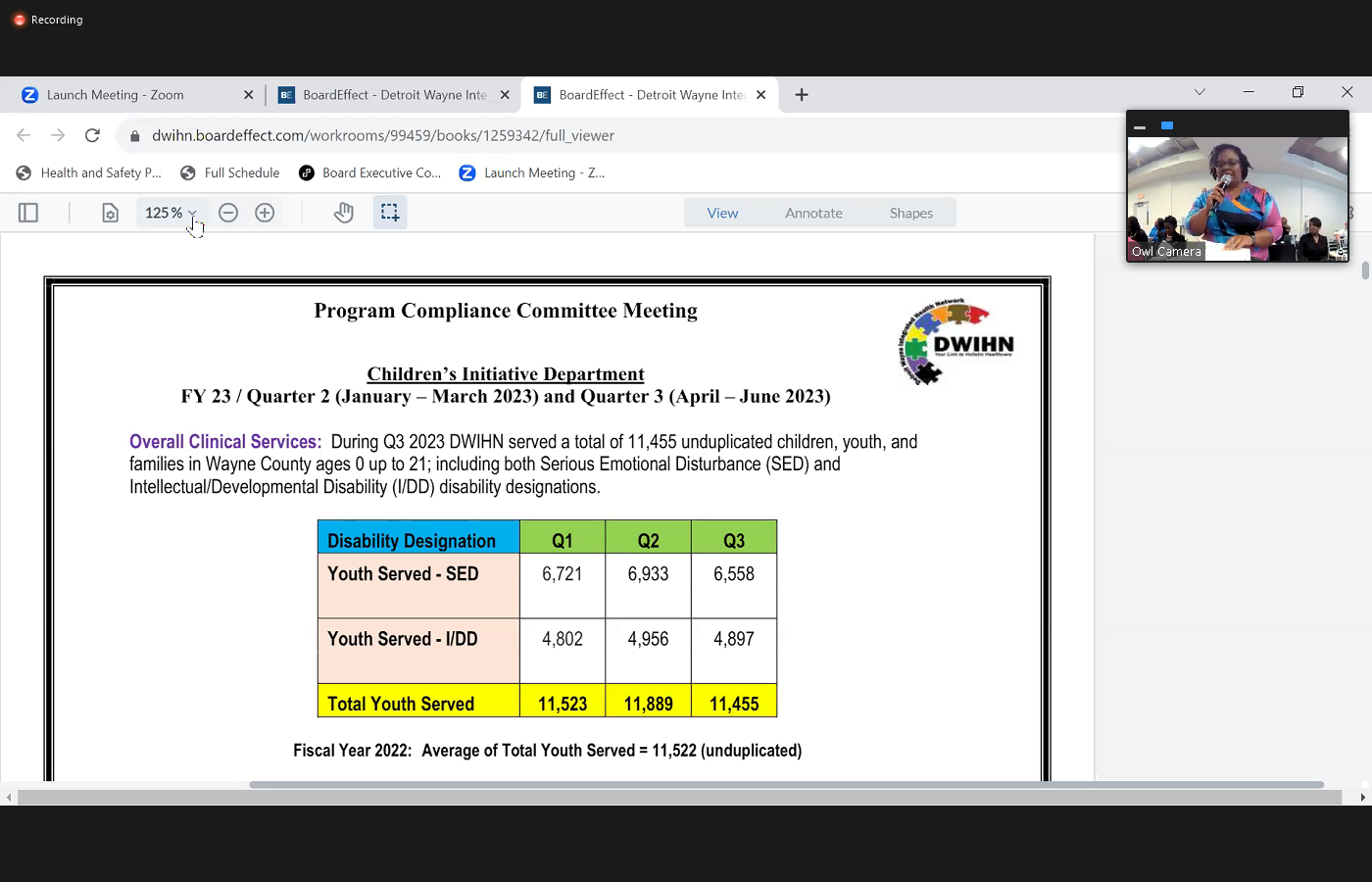
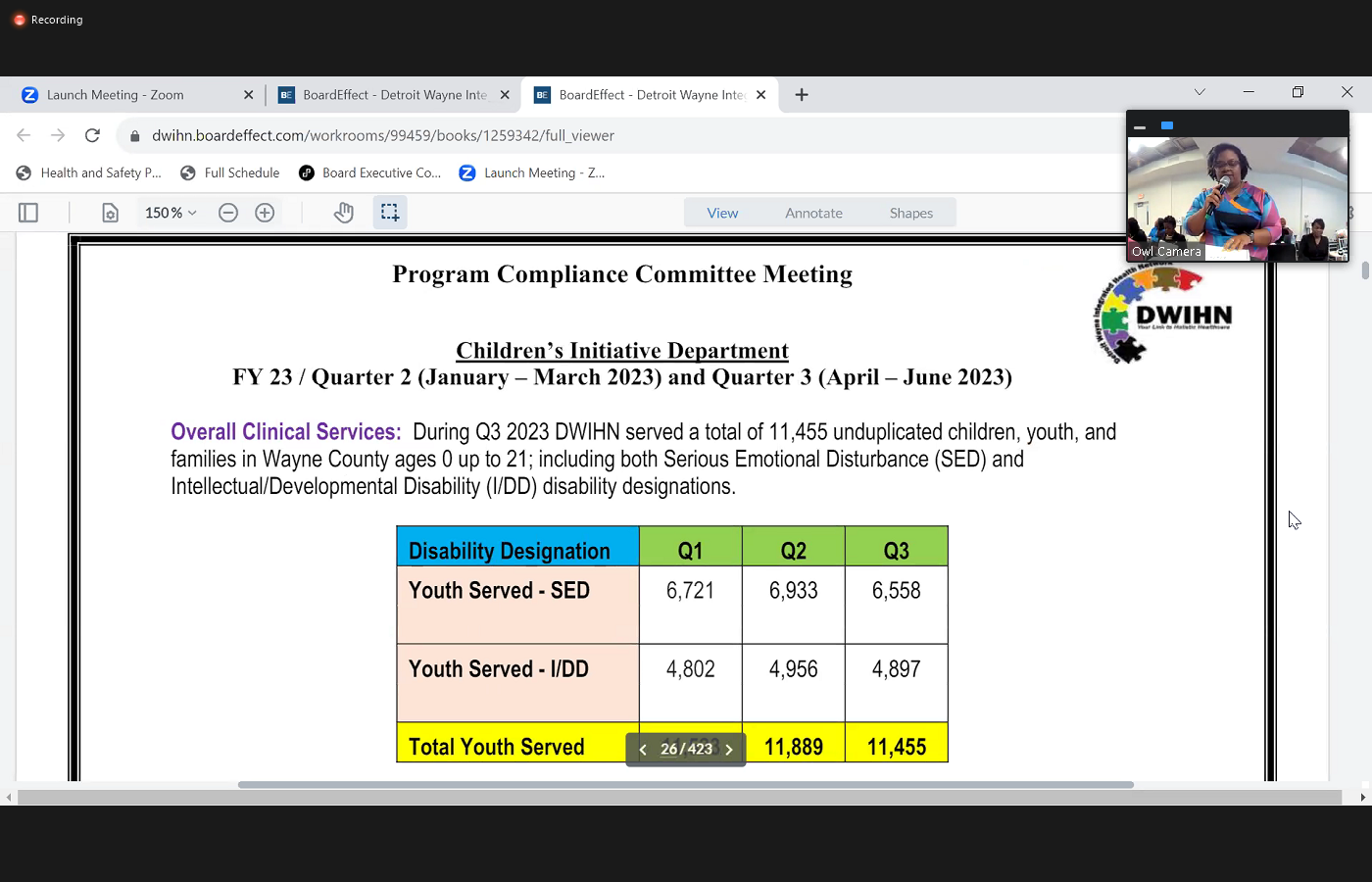 afternoon, everyone. I'm Cassandra cribs, Director of children's initiatives with Troy Wayne. I'm here to present the quarterly report. I'm actually going to be presenting on quarter two and quarter three. So that way you all hang in here the most current information, I will try to be as brief as the Yvonne was with hers. So for quarter, three overall, we served 11,485 unduplicated children, youth and families in Wayne County for ages zero to 21. That is for our youth with serious emotional disturbances known as sed and intellectual developmental disabilities known as IDD. There are three four, I'm sorry, there's three main activities. That has been a focus point for others, timely access to services juvenile restore to program and the School Success Initiative. So that will be the focus of today's presentation. Regarding timely access to service there's certain performance indicators that the state has identified, and we're doing well with the majority of them as we can see in the report. However, there's one in particular that we continue to have challenges with and that's access to services in completing that integrated bio cycle social assessment whenever there's a request and within 14 days, and
afternoon, everyone. I'm Cassandra cribs, Director of children's initiatives with Troy Wayne. I'm here to present the quarterly report. I'm actually going to be presenting on quarter two and quarter three. So that way you all hang in here the most current information, I will try to be as brief as the Yvonne was with hers. So for quarter, three overall, we served 11,485 unduplicated children, youth and families in Wayne County for ages zero to 21. That is for our youth with serious emotional disturbances known as sed and intellectual developmental disabilities known as IDD. There are three four, I'm sorry, there's three main activities. That has been a focus point for others, timely access to services juvenile restore to program and the School Success Initiative. So that will be the focus of today's presentation. Regarding timely access to service there's certain performance indicators that the state has identified, and we're doing well with the majority of them as we can see in the report. However, there's one in particular that we continue to have challenges with and that's access to services in completing that integrated bio cycle social assessment whenever there's a request and within 14 days, and 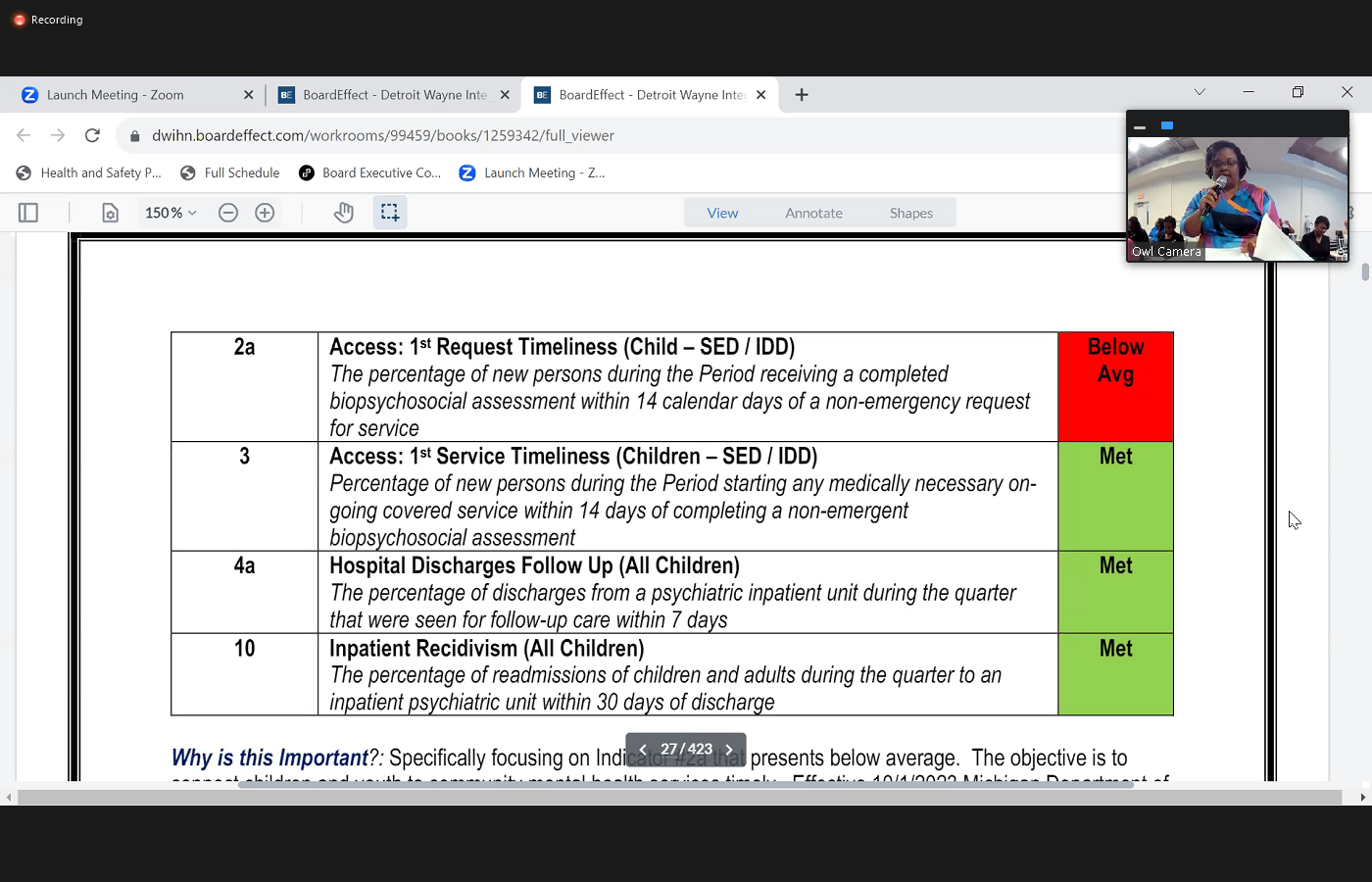
 so I have the data here to compare the different quarters also compared to last fiscal year. As well, and how we performed and as far as the accomplishment for quarter two, the youth with IDD that completed the intake within 14 days remain close to quarter one, meaning that there wasn't an decrease. The youth with sed completed an intake within 14 days was slightly increased by 5% compared to quarter one. Also, there were providers that were able to receive the value based incentive for IDD providers and FTD providers as well. And however we do continue to continue to work on the challenge of the intake assessment being completed within 14 days. We also are tracking even if it's not completing in 14 days, the percentage of the intake assessment still being completed. We do continue to meet with the providers to look at the barriers there is a monthly capacity form that providers are also completing. And then continuing to also brainstorm with the providers other solutions such as considering walking hours. You know, some of the feedback that we've been hearing is that there is availability to do intake assessments. However, they also want to
so I have the data here to compare the different quarters also compared to last fiscal year. As well, and how we performed and as far as the accomplishment for quarter two, the youth with IDD that completed the intake within 14 days remain close to quarter one, meaning that there wasn't an decrease. The youth with sed completed an intake within 14 days was slightly increased by 5% compared to quarter one. Also, there were providers that were able to receive the value based incentive for IDD providers and FTD providers as well. And however we do continue to continue to work on the challenge of the intake assessment being completed within 14 days. We also are tracking even if it's not completing in 14 days, the percentage of the intake assessment still being completed. We do continue to meet with the providers to look at the barriers there is a monthly capacity form that providers are also completing. And then continuing to also brainstorm with the providers other solutions such as considering walking hours. You know, some of the feedback that we've been hearing is that there is availability to do intake assessments. However, they also want to 
 make sure that there's enough staff to deliver the service after the intake has been completed. So some of our solutions of what we're doing in August we issued a request for proposal RFP. Also, there is one new provider that has submitted the application to the state to be a home based provider, which is a very much needed service right now. And then also come fiscal year 24 and October. All of the wraparound providers will also provide sed waiver services so that means that there will be an increase from five wraparound providers to nine wraparound and SED waiver providers. Regarding the juvenile restore to program this program, they actually started receiving referrals in July of 2023. This is a comprehensive service date a program at with teen wellness that provides individual group family therapy care management, supports educational supports food and transportation. And as of August 30 There were 15 youth enrolled in a program. However, as of today, there's actually 19 youth that are now enrolled in the program, and the majority of the youth are male participants. Also, we've had ongoing meetings with Team wellness regarding the program. Some accomplishments include that there was a gang unit from the Detroit Police Department that will come to the program to explain about gang activity and interventions. And, you know, there's also teen wellness is also was approved by Wayne County to develop an additional phase to offer therapeutic service to youth that are currently in JDF as well. We continue to address certain challenges and barriers such as you know, the education and safety of the students and the youth and also making sure that their school transcripts that are included and made available, as well for those that are in the program. So some of our plans moving forward is that we're going to continue to you know, make sure there's a streamlined process to the enrollment of the program. And also that the judges said that they will start including in the court order that they are to be able to get a copy of the school transcript as well that that is made available to Team wellness. And we actually there was actually a presentation with one of the local DHHS offices this Monday about the program and we continue to share information to the community about this program. And then also
make sure that there's enough staff to deliver the service after the intake has been completed. So some of our solutions of what we're doing in August we issued a request for proposal RFP. Also, there is one new provider that has submitted the application to the state to be a home based provider, which is a very much needed service right now. And then also come fiscal year 24 and October. All of the wraparound providers will also provide sed waiver services so that means that there will be an increase from five wraparound providers to nine wraparound and SED waiver providers. Regarding the juvenile restore to program this program, they actually started receiving referrals in July of 2023. This is a comprehensive service date a program at with teen wellness that provides individual group family therapy care management, supports educational supports food and transportation. And as of August 30 There were 15 youth enrolled in a program. However, as of today, there's actually 19 youth that are now enrolled in the program, and the majority of the youth are male participants. Also, we've had ongoing meetings with Team wellness regarding the program. Some accomplishments include that there was a gang unit from the Detroit Police Department that will come to the program to explain about gang activity and interventions. And, you know, there's also teen wellness is also was approved by Wayne County to develop an additional phase to offer therapeutic service to youth that are currently in JDF as well. We continue to address certain challenges and barriers such as you know, the education and safety of the students and the youth and also making sure that their school transcripts that are included and made available, as well for those that are in the program. So some of our plans moving forward is that we're going to continue to you know, make sure there's a streamlined process to the enrollment of the program. And also that the judges said that they will start including in the court order that they are to be able to get a copy of the school transcript as well that that is made available to Team wellness. And we actually there was actually a presentation with one of the local DHHS offices this Monday about the program and we continue to share information to the community about this program. And then also  in October, we have a joint meeting with the care management organizations, teen wellness, as well to talk to continue to do ongoing coordination. There were some board questions from the last meeting and I'm here to answer some of those regarding the demographics as I mentioned above, the majority of them are male regarding the gang activity. There. That information is looked at. Whenever they receive a referral they are looking at if there's any gang activity with the youth. It was reported that four other youth are involved in gangs and they there are safety measures included when it comes to transporting those youth as well, that those youth are not transported together. And as I mentioned, there's outside speakers that have come to Team moments to talk about gang activity regarding the student student teacher ratio currently is two to one and there is capacity to do the eight to one. Teacher to staff ups to student ratio. Also, regarding the conflict resolution, there's two evidence based practices that are provided cognitive behavioral therapy and aggression replacement training to address conflict resolution interventions. Also, the online schooling program as Keystone Academy and Kaplan GED prep. And the
in October, we have a joint meeting with the care management organizations, teen wellness, as well to talk to continue to do ongoing coordination. There were some board questions from the last meeting and I'm here to answer some of those regarding the demographics as I mentioned above, the majority of them are male regarding the gang activity. There. That information is looked at. Whenever they receive a referral they are looking at if there's any gang activity with the youth. It was reported that four other youth are involved in gangs and they there are safety measures included when it comes to transporting those youth as well, that those youth are not transported together. And as I mentioned, there's outside speakers that have come to Team moments to talk about gang activity regarding the student student teacher ratio currently is two to one and there is capacity to do the eight to one. Teacher to staff ups to student ratio. Also, regarding the conflict resolution, there's two evidence based practices that are provided cognitive behavioral therapy and aggression replacement training to address conflict resolution interventions. Also, the online schooling program as Keystone Academy and Kaplan GED prep. And the 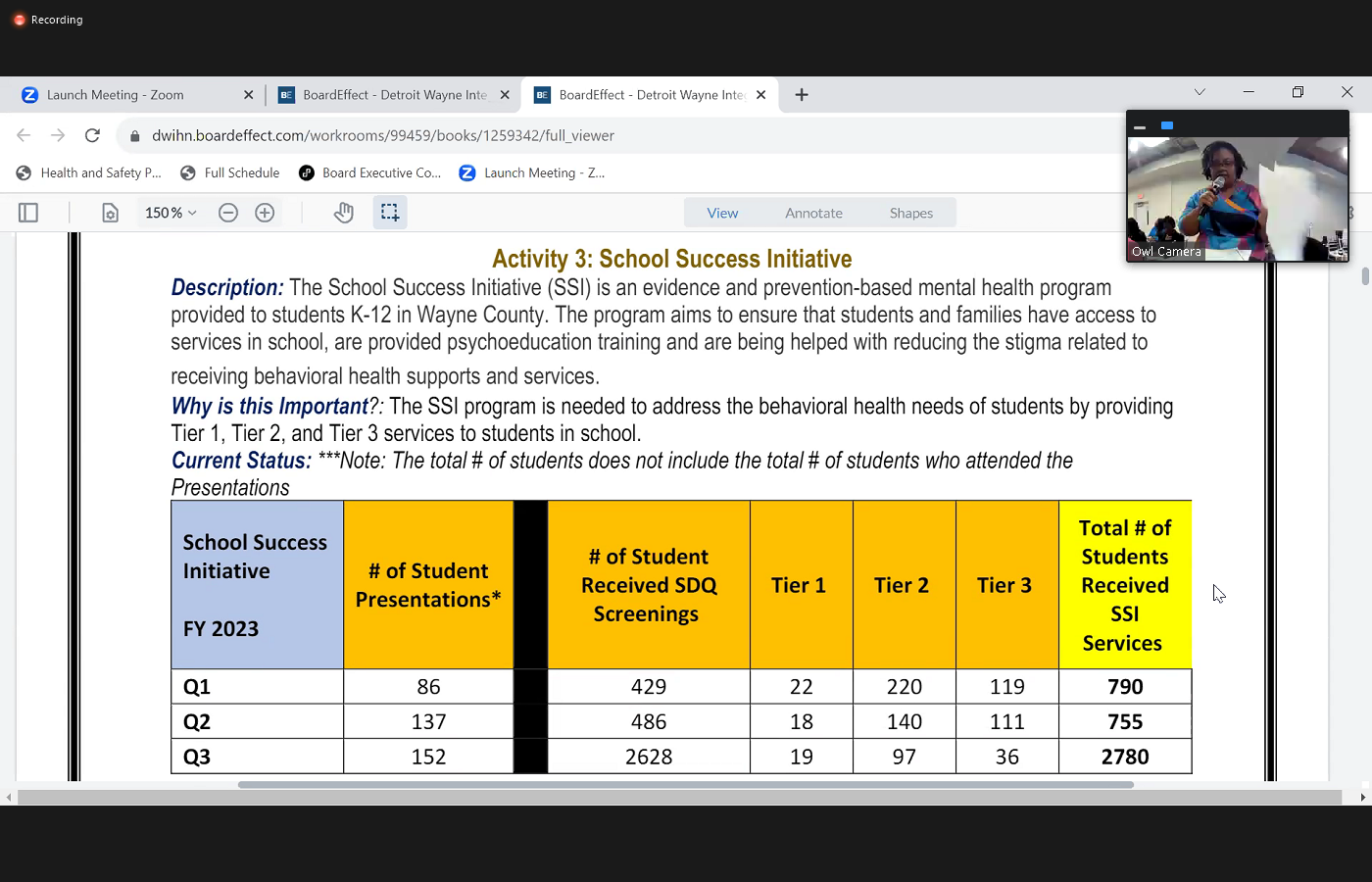
 regarding the cybersecurity the IT department do have firewall restrictions in place. And the youth do not have access to the information without permission and they are not allowed to bring their cell phones to the program regarding the outcomes that we're going to be looking at their services regarding like individual group Family Services, the school curriculum outcomes, and barriers. I'm flipping this page. Also looking at if they're successful, linkage to employment and skill building, and then also community reintegration outcomes as well. All right, next, the School Success Initiative. Regarding this, we're looking at quarters two and three. There was an increase of number of MCQ screenings which is the strength and difficulty scoring that was done from quarter to quarter three. And some of the major accomplishments is that there was also for quarter two discharges, successful discharges 81.5% were successful discharges, and there was also a decrease of the number of crisis screenings and hospitalizations from quarter two and quarter three as well. And there was an increase in the total number of students that receive services from quarter to quarter three, and we've been working on streamlining the the enrollment process and training the providers and also being able to do screenings. To get students enrolled in the program. And also, there was a request for information that was done to prepare for for school year 24. To answer the question regarding the prevention and versus the in depth services, so quarter a tiers one and two are more of those prevention and tier three is more the CMH and which is the community mental health services. So that's listed here on the chart. Not sure there's want me to provide a little bit more on that or was that enough to to answer your question?
regarding the cybersecurity the IT department do have firewall restrictions in place. And the youth do not have access to the information without permission and they are not allowed to bring their cell phones to the program regarding the outcomes that we're going to be looking at their services regarding like individual group Family Services, the school curriculum outcomes, and barriers. I'm flipping this page. Also looking at if they're successful, linkage to employment and skill building, and then also community reintegration outcomes as well. All right, next, the School Success Initiative. Regarding this, we're looking at quarters two and three. There was an increase of number of MCQ screenings which is the strength and difficulty scoring that was done from quarter to quarter three. And some of the major accomplishments is that there was also for quarter two discharges, successful discharges 81.5% were successful discharges, and there was also a decrease of the number of crisis screenings and hospitalizations from quarter two and quarter three as well. And there was an increase in the total number of students that receive services from quarter to quarter three, and we've been working on streamlining the the enrollment process and training the providers and also being able to do screenings. To get students enrolled in the program. And also, there was a request for information that was done to prepare for for school year 24. To answer the question regarding the prevention and versus the in depth services, so quarter a tiers one and two are more of those prevention and tier three is more the CMH and which is the community mental health services. So that's listed here on the chart. Not sure there's want me to provide a little bit more on that or was that enough to to answer your question?
+3
afternoon, everyone. I'm Cassandra cribs, Director of children's initiatives with Troy Wayne. I'm here to present the quarterly report. I'm actually going to be presenting on quarter two and quarter three. So that way you all hang in here the most current information, I will try to be as brief as the Yvonne was with hers. So for quarter, three overall, we served 11,485 unduplicated children, youth and families in Wayne County for ages zero to 21. That is for our youth with serious emotional disturbances known as sed and intellectual developmental disabilities known as IDD. There are three four, I'm sorry, there's three main activities. That has been a focus point for others, timely access to services juvenile restore to program and the School Success Initiative. So that will be the focus of today's presentation. Regarding timely access to service there's certain performance indicators that the state has identified, and we're doing well with the majority of them as we can see in the report. However, there's one in particular that we continue to have challenges with and that's access to services in completing that integrated bio cycle social assessment whenever there's a request and within 14 days, and 
+2
so I have the data here to compare the different quarters also compared to last fiscal year. As well, and how we performed and as far as the accomplishment for quarter two, the youth with IDD that completed the intake within 14 days remain close to quarter one, meaning that there wasn't an decrease. The youth with sed completed an intake within 14 days was slightly increased by 5% compared to quarter one. Also, there were providers that were able to receive the value based incentive for IDD providers and FTD providers as well. And however we do continue to continue to work on the challenge of the intake assessment being completed within 14 days. We also are tracking even if it's not completing in 14 days, the percentage of the intake assessment still being completed. We do continue to meet with the providers to look at the barriers there is a monthly capacity form that providers are also completing. And then continuing to also brainstorm with the providers other solutions such as considering walking hours. You know, some of the feedback that we've been hearing is that there is availability to do intake assessments. However, they also want to +2
make sure that there's enough staff to deliver the service after the intake has been completed. So some of our solutions of what we're doing in August we issued a request for proposal RFP. Also, there is one new provider that has submitted the application to the state to be a home based provider, which is a very much needed service right now. And then also come fiscal year 24 and October. All of the wraparound providers will also provide sed waiver services so that means that there will be an increase from five wraparound providers to nine wraparound and SED waiver providers. Regarding the juvenile restore to program this program, they actually started receiving referrals in July of 2023. This is a comprehensive service date a program at with teen wellness that provides individual group family therapy care management, supports educational supports food and transportation. And as of August 30 There were 15 youth enrolled in a program. However, as of today, there's actually 19 youth that are now enrolled in the program, and the majority of the youth are male participants. Also, we've had ongoing meetings with Team wellness regarding the program. Some accomplishments include that there was a gang unit from the Detroit Police Department that will come to the program to explain about gang activity and interventions. And, you know, there's also teen wellness is also was approved by Wayne County to develop an additional phase to offer therapeutic service to youth that are currently in JDF as well. We continue to address certain challenges and barriers such as you know, the education and safety of the students and the youth and also making sure that their school transcripts that are included and made available, as well for those that are in the program. So some of our plans moving forward is that we're going to continue to you know, make sure there's a streamlined process to the enrollment of the program. And also that the judges said that they will start including in the court order that they are to be able to get a copy of the school transcript as well that that is made available to Team wellness. And we actually there was actually a presentation with one of the local DHHS offices this Monday about the program and we continue to share information to the community about this program. And then also +1
in October, we have a joint meeting with the care management organizations, teen wellness, as well to talk to continue to do ongoing coordination. There were some board questions from the last meeting and I'm here to answer some of those regarding the demographics as I mentioned above, the majority of them are male regarding the gang activity. There. That information is looked at. Whenever they receive a referral they are looking at if there's any gang activity with the youth. It was reported that four other youth are involved in gangs and they there are safety measures included when it comes to transporting those youth as well, that those youth are not transported together. And as I mentioned, there's outside speakers that have come to Team moments to talk about gang activity regarding the student student teacher ratio currently is two to one and there is capacity to do the eight to one. Teacher to staff ups to student ratio. Also, regarding the conflict resolution, there's two evidence based practices that are provided cognitive behavioral therapy and aggression replacement training to address conflict resolution interventions. Also, the online schooling program as Keystone Academy and Kaplan GED prep. And the +2
regarding the cybersecurity the IT department do have firewall restrictions in place. And the youth do not have access to the information without permission and they are not allowed to bring their cell phones to the program regarding the outcomes that we're going to be looking at their services regarding like individual group Family Services, the school curriculum outcomes, and barriers. I'm flipping this page. Also looking at if they're successful, linkage to employment and skill building, and then also community reintegration outcomes as well. All right, next, the School Success Initiative. Regarding this, we're looking at quarters two and three. There was an increase of number of MCQ screenings which is the strength and difficulty scoring that was done from quarter to quarter three. And some of the major accomplishments is that there was also for quarter two discharges, successful discharges 81.5% were successful discharges, and there was also a decrease of the number of crisis screenings and hospitalizations from quarter two and quarter three as well. And there was an increase in the total number of students that receive services from quarter to quarter three, and we've been working on streamlining the the enrollment process and training the providers and also being able to do screenings. To get students enrolled in the program. And also, there was a request for information that was done to prepare for for school year 24. To answer the question regarding the prevention and versus the in depth services, so quarter a tiers one and two are more of those prevention and tier three is more the CMH and which is the community mental health services. So that's listed here on the chart. Not sure there's want me to provide a little bit more on that or was that enough to to answer your question? Unknown Speaker
You're looking at me. Yeah. I don't remember the question. Okay.
Speaker 4
Okay, so it must be enough. Okay. All right. All right. So the last thing I'll just say to some updates. We are preparing for the Mischa cans, which is launched we had the kickoff launch this week. And Wayne County is selected as a site for that. And this summer we've been doing a lot of great activities, Detroit computers, we did another one with the Children's Center. There were 36 attendees for that. And there's been a variety of different interviews to prepare for back to school this summer as well. We've been working with the providers on improvement crisis plan and then also our PHA has been a lot of improvement as well we've increased to now we're averaging at 78% compliance with PHQ as we compare to last year after da percent. So that concludes my report.
Unknown Speaker
Are there any questions? That's Carter?
Speaker 9
Just a brief question. I'm trying to understand how to read the chart where you compare quarter to summary and quarter three, are those discrete times or kids can be in both quarters.
Speaker 4
Regarding the school six which program Yes. Okay, excess,
Speaker 9
because as I look at quarter three, the number of referrals is much less than the number of discharges. So does that tell me that kids can be in multiple quarters?
Speaker 4
So what happens is, is that at the beginning of the school year, they issue that MCQ screening is issued at the beginning of the year, however they can receive those all throughout the year. And so the referral number can fluctuate throughout the year and then also completion of the other program can fluctuate throughout the year as well.
Speaker 9
So how should I interpret the risk factors? Are those discrete to that quarter or does that fluctuate? I look at bullying for for instance and 64 in quarter two and 33. Could a child still have billing issues throughout the year and you would mark them for each quarter?
Speaker 4
So where it has the risk factors those are actually the number of presentations that were done. Okay.
Unknown Speaker
That, yeah,
Speaker 7
yeah, just um, and I'll try to remember this question. But in the juvenile restorative program, do they have any program that deals with black history are understanding their past and, and understand some of the reasons why they may be in gangs and things of that nature?
Speaker 4
That's a wonderful question, Mr. Parker, and I can definitely look into that further for you.
Unknown Speaker
I'm gonna make sure I remember it when you come
Unknown Speaker
back. Thank you. Thank you. Miss Bullock. Yeah.
Speaker 8
Thank you, Madam Chair. My question is tied to the same program, the team wellness. I'm wondering how our current census compares to the projections or is there any concern I mean, I know that there's work to make sure they're getting their referrals, but how does it compare to what we thought we'd have at this time?
Speaker 4
So that we started, they started receiving referrals in July, and the maximum capacity is 70. And so right now they're at 19. They're also looking at expanding their, their location, their space as well, to add more. And then also there's been a lot of communication with the judges still education to the community about the program, because some judges are still not as aware or so we actually when we met with teen wellness recently talked about sending communication to the judges so that they are aware that they know that there's capacity for the program and regarding sending referrals, so we continue to do that, that coordination and that linkage as well. With the with the court system, and I'm not sure Melissa wants to answer that chair.
Speaker 1
Yeah. Um, so that was okay. Yes. Go ahead, Melissa.
Speaker 15
Thank you. I'm Melissa moody, VP of Clinical Operations. Just to add to that, we did actually meet with Team wellness today to talk about this, this very fact of the referrals and what we did find out is some of the judges that process these referrals. Somehow got some sort of communication, we're not sure where that the program was at capacity. And so we want to make sure that the judges are aware we are we are definitely not at capacity at this point. So we're sending a memo and having some communications during our upcoming meetings with the judicial system to make sure that we they are aware of it and we're going to be sending teams going to be sending an ongoing correspondence on a weekly basis to indicate what their capacity is to them so they continue to get the appropriate referrals.
Speaker 1
Okay, I have one comment for you. Out School Success Initiative. Yes. So there's a statewide association of school based health centers. There's a national association, they have an annual conference. I really think the work that you're doing is very exemplary. And is is inspirational. So I would like you all to consider reaching out to do a presentation, either the national conference or their state. I don't know if they have a statewide conference, but there is a statewide association. I just like them to be really aware of the work that you're doing around school success and some of the outcomes that you're having. So, again, it's just a recommendation that you reach out. Yes, definitely. And present to them or what the work that you're doing.
Unknown Speaker
Okay. Yes.
Speaker 1
All right. Any further questions? All right. All right. Thank you so much for Thank you. You guys are doing a great job. All right. So we'll now hear from customer service, I think it is yes.
Speaker 16
Good 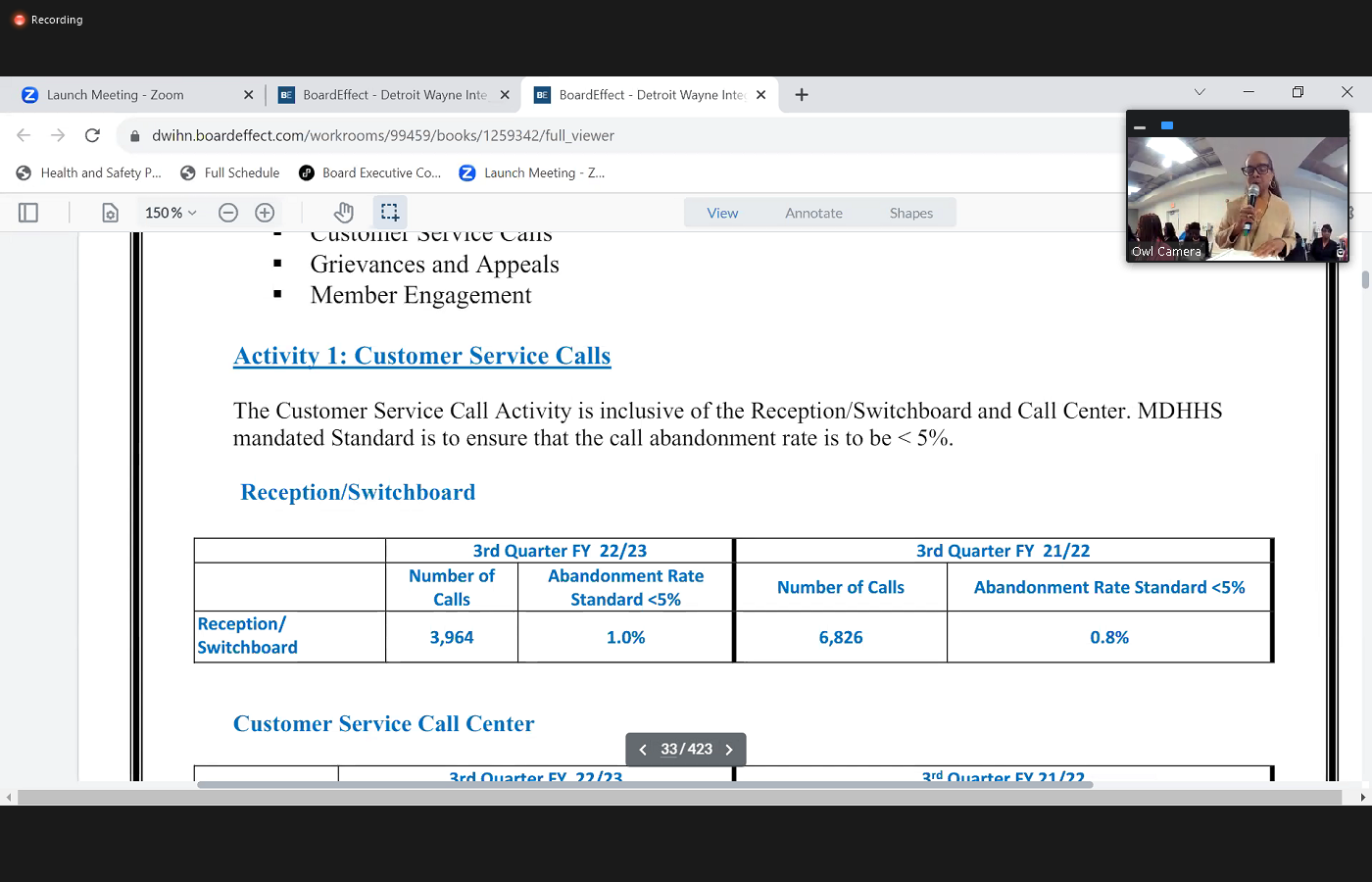
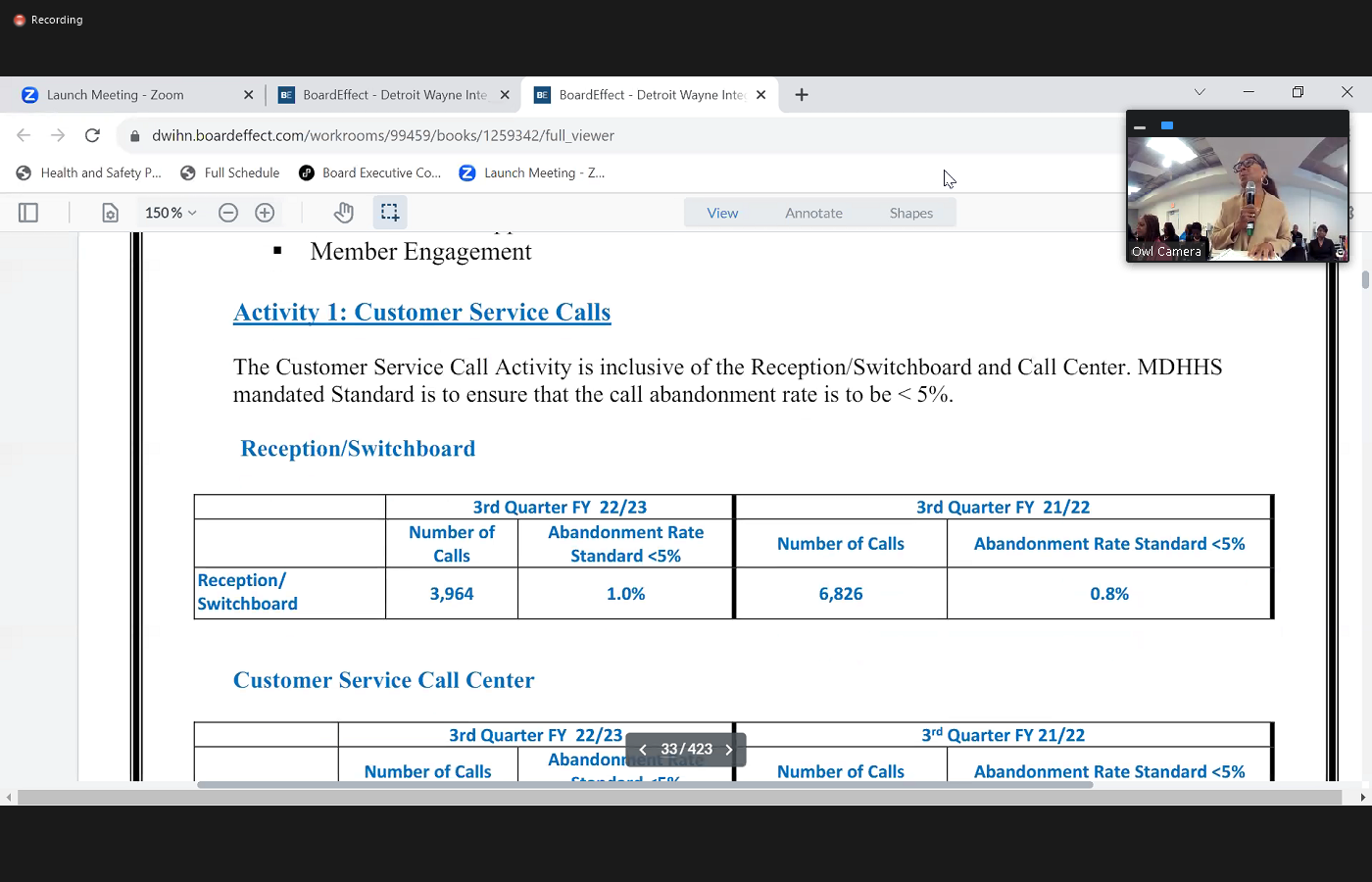 afternoon, Madam Chair and fellow board members. I'm Michele FastCAM. Sell us I'm the director of customer service. And I am going to be focusing on third quarter reporting on three particular areas and that'll be customer service calls. grievances and appeals as well as member engagement. Okay, our first activity is in reference to customer service calls. And here, our activity includes our switchboard reception area, as well as our call center. And as you know, the mandate for abandonment rate is less than 5% that the state has given us. So with our switchboard, we looked at a little bit less than 4000 calls that came in in this third quarter with an abandonment rate of 1.0%. So we were glad about that. Our third quarter from the previous fiscal year though, we had a significantly larger number of 6826 calls that came in and we had a man rate of 0.8%. So again, still well within our compliance. When we looked at our Customer Service Call Center, we did have 1436 calls that came in to our third quarter of this fiscal year with a 3.1% Abandon rate. When we compare that to fiscal year of 2122.
afternoon, Madam Chair and fellow board members. I'm Michele FastCAM. Sell us I'm the director of customer service. And I am going to be focusing on third quarter reporting on three particular areas and that'll be customer service calls. grievances and appeals as well as member engagement. Okay, our first activity is in reference to customer service calls. And here, our activity includes our switchboard reception area, as well as our call center. And as you know, the mandate for abandonment rate is less than 5% that the state has given us. So with our switchboard, we looked at a little bit less than 4000 calls that came in in this third quarter with an abandonment rate of 1.0%. So we were glad about that. Our third quarter from the previous fiscal year though, we had a significantly larger number of 6826 calls that came in and we had a man rate of 0.8%. So again, still well within our compliance. When we looked at our Customer Service Call Center, we did have 1436 calls that came in to our third quarter of this fiscal year with a 3.1% Abandon rate. When we compare that to fiscal year of 2122.  However, we did have a significantly larger number of calls, yet we had an abandonment rate of 7.5%, which was 2%. Over and that was really in reference to some issues that we were having in terms of staffing, as well as some technical problems. And we have since resolved that in addition to that, we actually posted some positions and had those filled and then we worked with our IT department in terms of some of those problems. We were having some technical issues. So those have since been resolved. One of the things that was mentioned earlier was that you know, we are looking at a new phone system, so we've identified that particular vendor, but during the course of the third fiscal year, we were actually going through the evaluation process and so customer service was part of that evaluation team as well as our IT department procurement, and also our Access Center. Also in the area of customer service and trying to make sure that we address any type of abandonment, right because we know that with staffing issues, you have people that go on vacations, you have PTO, and what have you and so we've
However, we did have a significantly larger number of calls, yet we had an abandonment rate of 7.5%, which was 2%. Over and that was really in reference to some issues that we were having in terms of staffing, as well as some technical problems. And we have since resolved that in addition to that, we actually posted some positions and had those filled and then we worked with our IT department in terms of some of those problems. We were having some technical issues. So those have since been resolved. One of the things that was mentioned earlier was that you know, we are looking at a new phone system, so we've identified that particular vendor, but during the course of the third fiscal year, we were actually going through the evaluation process and so customer service was part of that evaluation team as well as our IT department procurement, and also our Access Center. Also in the area of customer service and trying to make sure that we address any type of abandonment, right because we know that with staffing issues, you have people that go on vacations, you have PTO, and what have you and so we've  done some cross training at our department for individuals to backup that system. If we need additional phone coverage. Our second area is in the area of grievances and appeals. And here we want to make sure that our members are ensure that they're provided they're a means to due process. And so in this area, we deal with complaints, grievances, appeals, mediation, estate fair hearings, and so what you'll find in our first data in terms of related communications, with our complaints and grievances, you'll see that that number is 709. And that is actually encounters that we dealt with and when we find encounters we're looking at in terms of calls as well as follow up calls that we have to make to address that complaint, as well as any type of referral we oftentimes get complaints from the state. And so we have to make multiple calls or do some collaboration with departments. So you'll see that that number looks extremely large compared to the previous quarter where we were actually just reporting on on calls that were coming in and so we made this change because my team wanted to show their real productivity in terms
done some cross training at our department for individuals to backup that system. If we need additional phone coverage. Our second area is in the area of grievances and appeals. And here we want to make sure that our members are ensure that they're provided they're a means to due process. And so in this area, we deal with complaints, grievances, appeals, mediation, estate fair hearings, and so what you'll find in our first data in terms of related communications, with our complaints and grievances, you'll see that that number is 709. And that is actually encounters that we dealt with and when we find encounters we're looking at in terms of calls as well as follow up calls that we have to make to address that complaint, as well as any type of referral we oftentimes get complaints from the state. And so we have to make multiple calls or do some collaboration with departments. So you'll see that that number looks extremely large compared to the previous quarter where we were actually just reporting on on calls that were coming in and so we made this change because my team wanted to show their real productivity in terms 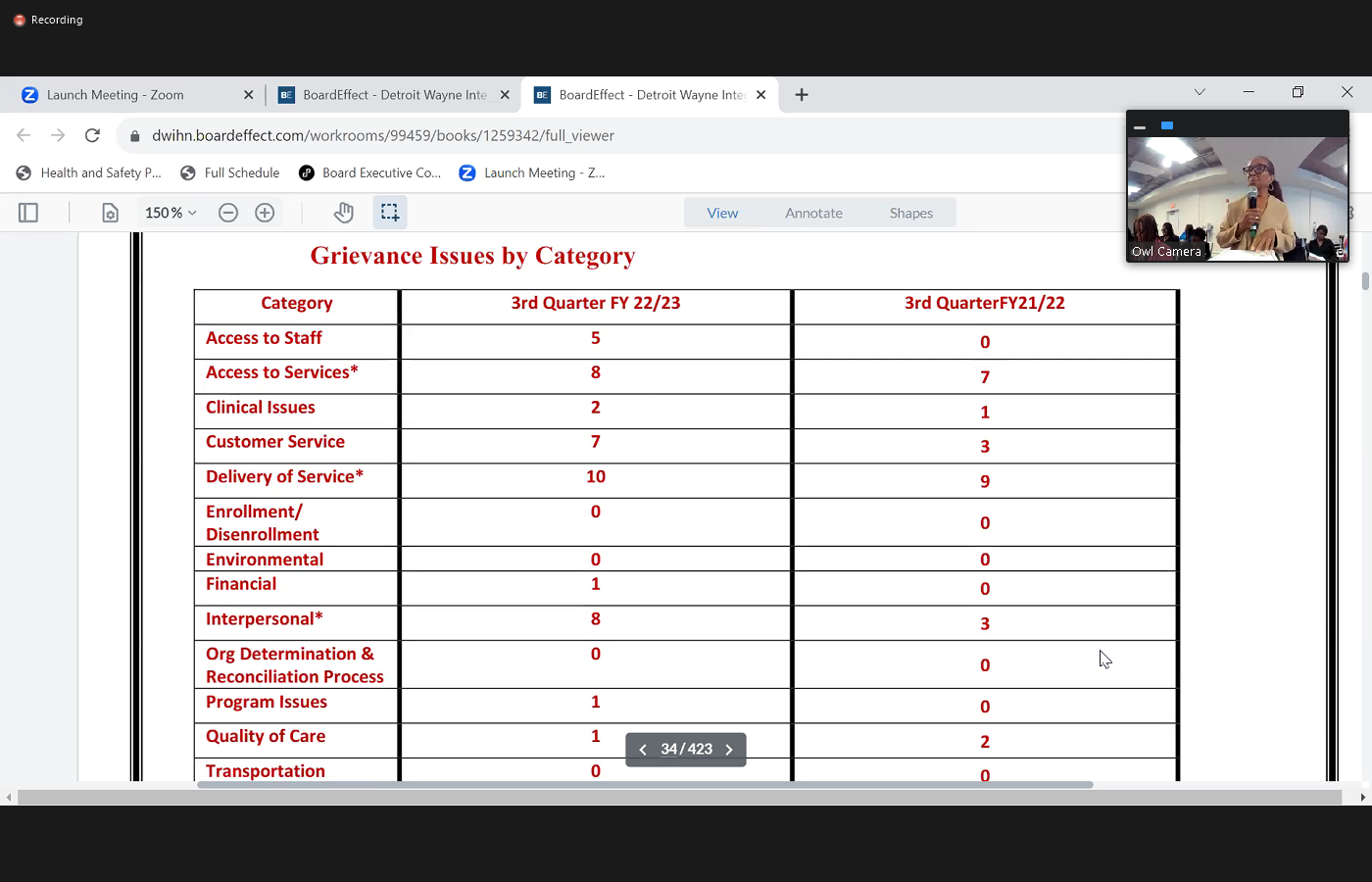
 of addressing issues and so that actually happened and bid 2122 are in terms of the actual grievances that were processed with the quarterly comparison. We had about 27 that we received in the third quarter for fiscal year 20 to 23. And we actually resolved 25 of those in the third quarter fiscal year. 2122 was a little bit smaller numbers of 20 and 19. When you look at our next chart there, we're talking about the grievances and a grievance can have more than one issue. And so we identify all categories that that grievance may have fallen into. And so what you'll see is that we had a total of 45 that were actually in the first the third question, third fiscal year for 2022 23. And we actually have 32 for the third quarter of 2122. We'd like to be able to focus in on some of the key areas that we're showing a pattern. And so what you'll see in fiscal year 2223, the three categories that we've identified, is that we have the delivery of service as being a key area that we had about 10 that fell in that category and then we had access to I'm sorry, interpersonal relationships, complaints as a second category and then access to services in comparison to the previous fiscal year. Again, delivery of services was a concern as the first area and then also we had access to services, this being our second category and then White time. What we have done is that we try to look at these areas in these trends and patterns then, and there's been certain initiatives that Dewayne has taken in terms of we have an access committee now where we address access to care issues and and so we report on that on a monthly basis and try to look at where there's some areas that we can focus on for process improvements. In the past we have done this is prior to COVID when we identified there was a complaint in terms of a crisp provider that's having a waiting time issue people are waiting in the waiting room before they can be seen. We actually took customer service staff and did some mystery shopping and set out there in the lobby in an observation so we are looking at ways to address process improvement. I apologize I'm all
of addressing issues and so that actually happened and bid 2122 are in terms of the actual grievances that were processed with the quarterly comparison. We had about 27 that we received in the third quarter for fiscal year 20 to 23. And we actually resolved 25 of those in the third quarter fiscal year. 2122 was a little bit smaller numbers of 20 and 19. When you look at our next chart there, we're talking about the grievances and a grievance can have more than one issue. And so we identify all categories that that grievance may have fallen into. And so what you'll see is that we had a total of 45 that were actually in the first the third question, third fiscal year for 2022 23. And we actually have 32 for the third quarter of 2122. We'd like to be able to focus in on some of the key areas that we're showing a pattern. And so what you'll see in fiscal year 2223, the three categories that we've identified, is that we have the delivery of service as being a key area that we had about 10 that fell in that category and then we had access to I'm sorry, interpersonal relationships, complaints as a second category and then access to services in comparison to the previous fiscal year. Again, delivery of services was a concern as the first area and then also we had access to services, this being our second category and then White time. What we have done is that we try to look at these areas in these trends and patterns then, and there's been certain initiatives that Dewayne has taken in terms of we have an access committee now where we address access to care issues and and so we report on that on a monthly basis and try to look at where there's some areas that we can focus on for process improvements. In the past we have done this is prior to COVID when we identified there was a complaint in terms of a crisp provider that's having a waiting time issue people are waiting in the waiting room before they can be seen. We actually took customer service staff and did some mystery shopping and set out there in the lobby in an observation so we are looking at ways to address process improvement. I apologize I'm all 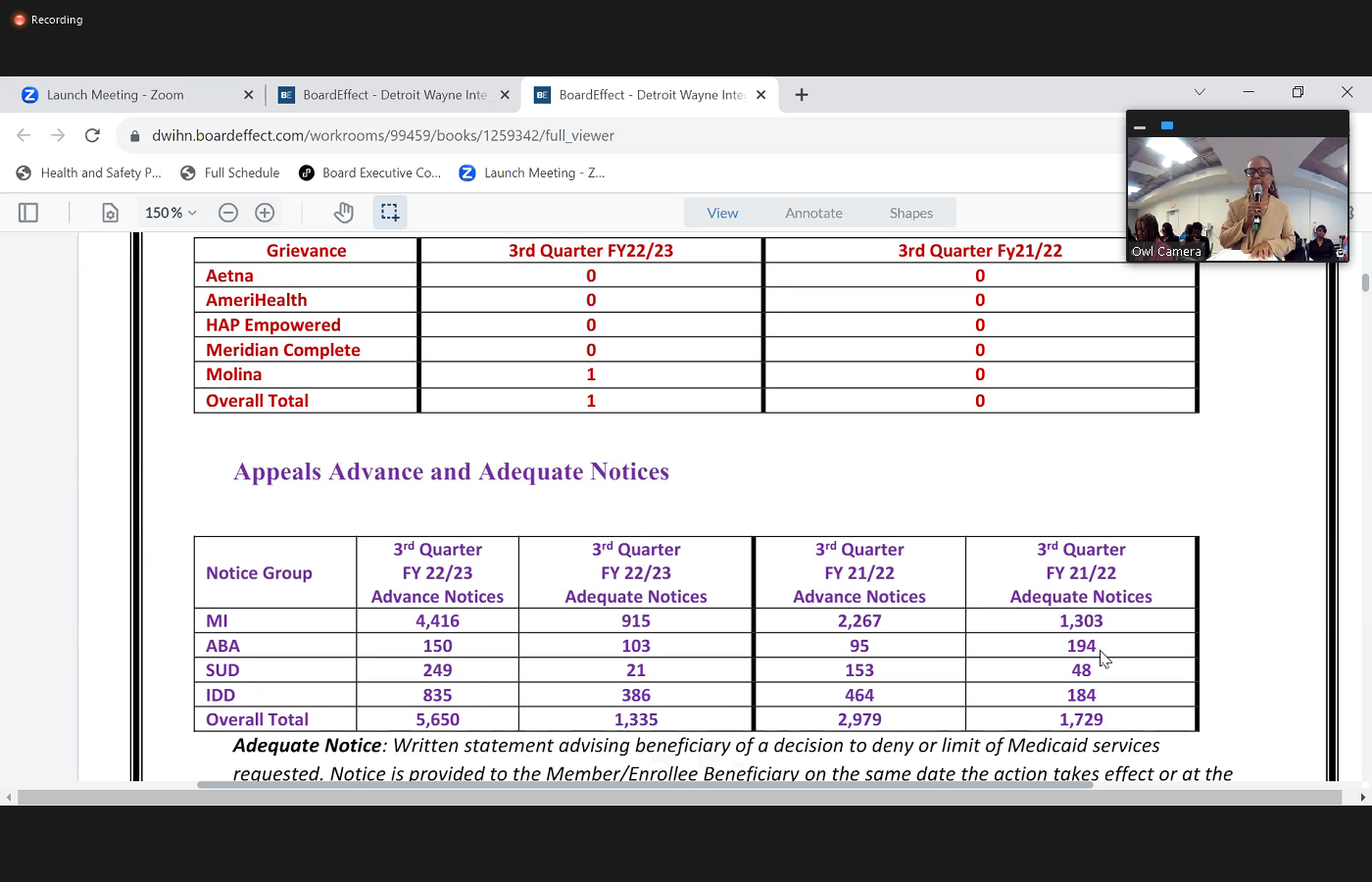
 those. Also, we have our my Healthlink demonstration project where we also have to record grievances. And what we find is that routinely is it's been rare that we've had, sir. It's been rare that we've had more than two grievances and a court for that. And so what you'll find with this third quarter, we only had one and that was with our Molina health plan and then the third quarter of previous fiscal year there were absolutely absolutely no. As you'll also see in terms of my next category, which talks about appeals, which is also another due process, you'll see that we've had a significant increase in the number of advance notices as well as our adequate notices compared to the previous fiscal year. What you need to know is that provider if he decides to deny or limit Medicaid services, he has to issue a notice to that member. The same thing calls for if there's a decision to reduce suspend or terminate a service. They have to issue an adequate advance notice. And so what happens is with that particular notice that goes out explains to them the members rights to an appeal, and so they are instructed to contact our customer service department. We actually are looking at trends and patterns. And we're also doing some auditing to make sure that our providers are following the appropriate process that they've given the adequate notice to these individuals. And so that's what we're tracking here. We also looked at, again, appeals communications and we took the same thought in terms of identifying all all activity that is involved in resolving those appeals. And so you'll see that we had 431 In our third quarter of this fiscal year and then actually 81 calls that was
those. Also, we have our my Healthlink demonstration project where we also have to record grievances. And what we find is that routinely is it's been rare that we've had, sir. It's been rare that we've had more than two grievances and a court for that. And so what you'll find with this third quarter, we only had one and that was with our Molina health plan and then the third quarter of previous fiscal year there were absolutely absolutely no. As you'll also see in terms of my next category, which talks about appeals, which is also another due process, you'll see that we've had a significant increase in the number of advance notices as well as our adequate notices compared to the previous fiscal year. What you need to know is that provider if he decides to deny or limit Medicaid services, he has to issue a notice to that member. The same thing calls for if there's a decision to reduce suspend or terminate a service. They have to issue an adequate advance notice. And so what happens is with that particular notice that goes out explains to them the members rights to an appeal, and so they are instructed to contact our customer service department. We actually are looking at trends and patterns. And we're also doing some auditing to make sure that our providers are following the appropriate process that they've given the adequate notice to these individuals. And so that's what we're tracking here. We also looked at, again, appeals communications and we took the same thought in terms of identifying all all activity that is involved in resolving those appeals. And so you'll see that we had 431 In our third quarter of this fiscal year and then actually 81 calls that was 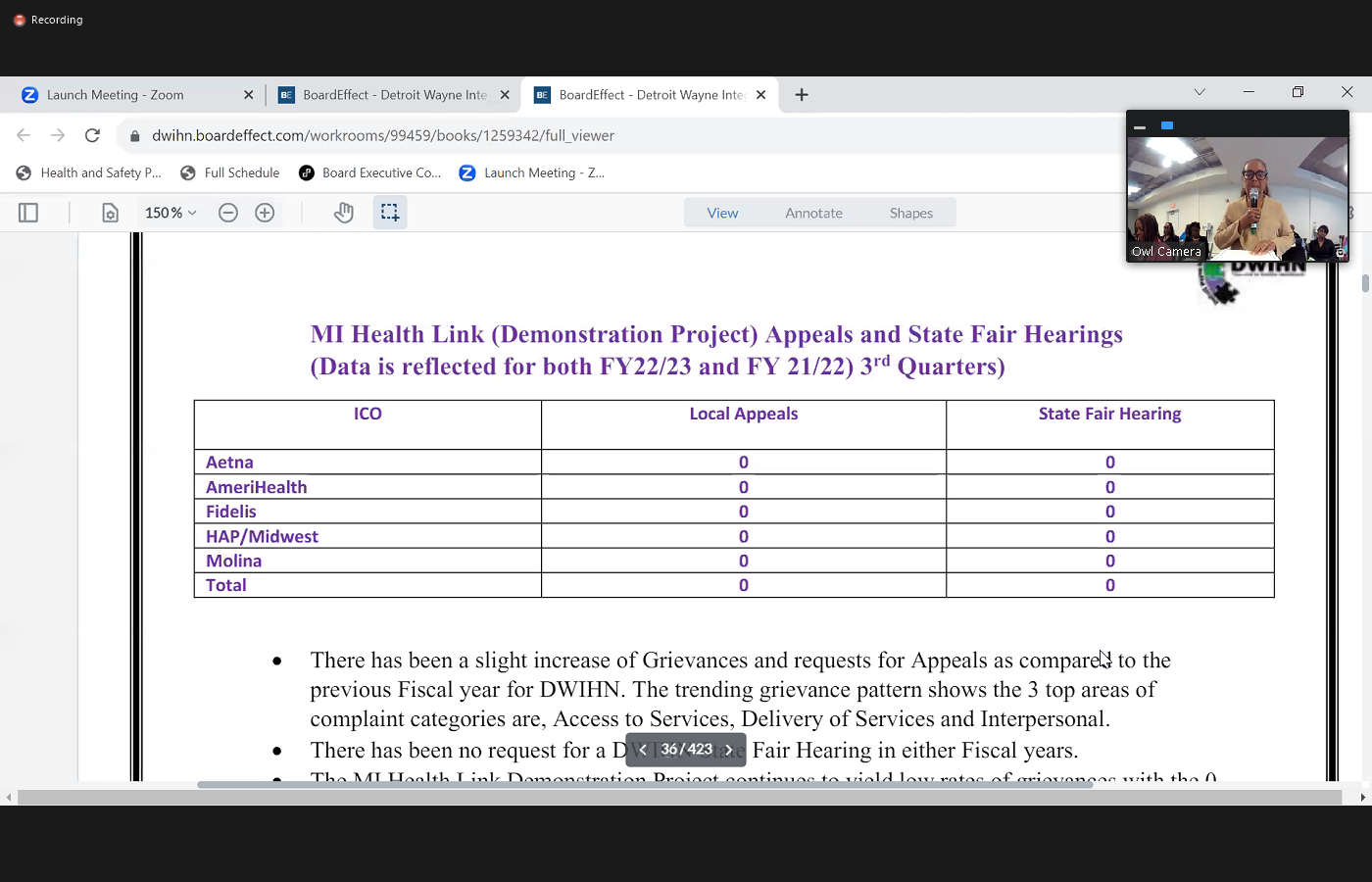
 in our previous fiscal year. Actual appeals that we receive are about 18 for I'm sorry, 16 For our third quarter, and those that were resolvable, 14 And our third quarter of fiscal year 2122 is a little bit less. You'll find that our staff here hearings, we seem to be staying at a zero rate in terms of the requests for a state fair hearing. And that also holds true for our my Healthlink program. Some of the initiatives that we have actually been looking at is that we have customer service quarterly provider meetings and this gives us an opportunity to focus on updates as well as focus on grievances appeals, and some of the things that we're identifying areas that need process improvements. One of the things that we have noticed with with just a small number of our our grievance our providers in refers to grievances is that they're trying to develop an internal process to resolve grievances and circumvent us altogether. And so we're not having that and so we're actually addressing those kinds of issues and, and trying to make sure through technical assistance that when we get this resolved before we have to take it any further into compliance issue. Another thing is that
in our previous fiscal year. Actual appeals that we receive are about 18 for I'm sorry, 16 For our third quarter, and those that were resolvable, 14 And our third quarter of fiscal year 2122 is a little bit less. You'll find that our staff here hearings, we seem to be staying at a zero rate in terms of the requests for a state fair hearing. And that also holds true for our my Healthlink program. Some of the initiatives that we have actually been looking at is that we have customer service quarterly provider meetings and this gives us an opportunity to focus on updates as well as focus on grievances appeals, and some of the things that we're identifying areas that need process improvements. One of the things that we have noticed with with just a small number of our our grievance our providers in refers to grievances is that they're trying to develop an internal process to resolve grievances and circumvent us altogether. And so we're not having that and so we're actually addressing those kinds of issues and, and trying to make sure through technical assistance that when we get this resolved before we have to take it any further into compliance issue. Another thing is that
+3
afternoon, Madam Chair and fellow board members. I'm Michele FastCAM. Sell us I'm the director of customer service. And I am going to be focusing on third quarter reporting on three particular areas and that'll be customer service calls. grievances and appeals as well as member engagement. Okay, our first activity is in reference to customer service calls. And here, our activity includes our switchboard reception area, as well as our call center. And as you know, the mandate for abandonment rate is less than 5% that the state has given us. So with our switchboard, we looked at a little bit less than 4000 calls that came in in this third quarter with an abandonment rate of 1.0%. So we were glad about that. Our third quarter from the previous fiscal year though, we had a significantly larger number of 6826 calls that came in and we had a man rate of 0.8%. So again, still well within our compliance. When we looked at our Customer Service Call Center, we did have 1436 calls that came in to our third quarter of this fiscal year with a 3.1% Abandon rate. When we compare that to fiscal year of 2122. 
+1
However, we did have a significantly larger number of calls, yet we had an abandonment rate of 7.5%, which was 2%. Over and that was really in reference to some issues that we were having in terms of staffing, as well as some technical problems. And we have since resolved that in addition to that, we actually posted some positions and had those filled and then we worked with our IT department in terms of some of those problems. We were having some technical issues. So those have since been resolved. One of the things that was mentioned earlier was that you know, we are looking at a new phone system, so we've identified that particular vendor, but during the course of the third fiscal year, we were actually going through the evaluation process and so customer service was part of that evaluation team as well as our IT department procurement, and also our Access Center. Also in the area of customer service and trying to make sure that we address any type of abandonment, right because we know that with staffing issues, you have people that go on vacations, you have PTO, and what have you and so we've +1
done some cross training at our department for individuals to backup that system. If we need additional phone coverage. Our second area is in the area of grievances and appeals. And here we want to make sure that our members are ensure that they're provided they're a means to due process. And so in this area, we deal with complaints, grievances, appeals, mediation, estate fair hearings, and so what you'll find in our first data in terms of related communications, with our complaints and grievances, you'll see that that number is 709. And that is actually encounters that we dealt with and when we find encounters we're looking at in terms of calls as well as follow up calls that we have to make to address that complaint, as well as any type of referral we oftentimes get complaints from the state. And so we have to make multiple calls or do some collaboration with departments. So you'll see that that number looks extremely large compared to the previous quarter where we were actually just reporting on on calls that were coming in and so we made this change because my team wanted to show their real productivity in terms +2
of addressing issues and so that actually happened and bid 2122 are in terms of the actual grievances that were processed with the quarterly comparison. We had about 27 that we received in the third quarter for fiscal year 20 to 23. And we actually resolved 25 of those in the third quarter fiscal year. 2122 was a little bit smaller numbers of 20 and 19. When you look at our next chart there, we're talking about the grievances and a grievance can have more than one issue. And so we identify all categories that that grievance may have fallen into. And so what you'll see is that we had a total of 45 that were actually in the first the third question, third fiscal year for 2022 23. And we actually have 32 for the third quarter of 2122. We'd like to be able to focus in on some of the key areas that we're showing a pattern. And so what you'll see in fiscal year 2223, the three categories that we've identified, is that we have the delivery of service as being a key area that we had about 10 that fell in that category and then we had access to I'm sorry, interpersonal relationships, complaints as a second category and then access to services in comparison to the previous fiscal year. Again, delivery of services was a concern as the first area and then also we had access to services, this being our second category and then White time. What we have done is that we try to look at these areas in these trends and patterns then, and there's been certain initiatives that Dewayne has taken in terms of we have an access committee now where we address access to care issues and and so we report on that on a monthly basis and try to look at where there's some areas that we can focus on for process improvements. In the past we have done this is prior to COVID when we identified there was a complaint in terms of a crisp provider that's having a waiting time issue people are waiting in the waiting room before they can be seen. We actually took customer service staff and did some mystery shopping and set out there in the lobby in an observation so we are looking at ways to address process improvement. I apologize I'm all +2
those. Also, we have our my Healthlink demonstration project where we also have to record grievances. And what we find is that routinely is it's been rare that we've had, sir. It's been rare that we've had more than two grievances and a court for that. And so what you'll find with this third quarter, we only had one and that was with our Molina health plan and then the third quarter of previous fiscal year there were absolutely absolutely no. As you'll also see in terms of my next category, which talks about appeals, which is also another due process, you'll see that we've had a significant increase in the number of advance notices as well as our adequate notices compared to the previous fiscal year. What you need to know is that provider if he decides to deny or limit Medicaid services, he has to issue a notice to that member. The same thing calls for if there's a decision to reduce suspend or terminate a service. They have to issue an adequate advance notice. And so what happens is with that particular notice that goes out explains to them the members rights to an appeal, and so they are instructed to contact our customer service department. We actually are looking at trends and patterns. And we're also doing some auditing to make sure that our providers are following the appropriate process that they've given the adequate notice to these individuals. And so that's what we're tracking here. We also looked at, again, appeals communications and we took the same thought in terms of identifying all all activity that is involved in resolving those appeals. And so you'll see that we had 431 In our third quarter of this fiscal year and then actually 81 calls that was +2
in our previous fiscal year. Actual appeals that we receive are about 18 for I'm sorry, 16 For our third quarter, and those that were resolvable, 14 And our third quarter of fiscal year 2122 is a little bit less. You'll find that our staff here hearings, we seem to be staying at a zero rate in terms of the requests for a state fair hearing. And that also holds true for our my Healthlink program. Some of the initiatives that we have actually been looking at is that we have customer service quarterly provider meetings and this gives us an opportunity to focus on updates as well as focus on grievances appeals, and some of the things that we're identifying areas that need process improvements. One of the things that we have noticed with with just a small number of our our grievance our providers in refers to grievances is that they're trying to develop an internal process to resolve grievances and circumvent us altogether. And so we're not having that and so we're actually addressing those kinds of issues and, and trying to make sure through technical assistance that when we get this resolved before we have to take it any further into compliance issue. Another thing is that Unknown Speaker
highlights I
Unknown Speaker
I'm gonna move on to our third activity
Speaker 1
every day and we do we do have the report so we know you're doing a good job. Just the highlights. Okay.
Speaker 16
Yeah. I always think I'm shorter this time. Okay, I'm sorry, the member experience. We have lots of stuff that's going on with our member experience. In fact, today we're at walk a mile in my students then watching me go, Lansing, and Lansing, and we're going to be well represented there on the Capitol. And so, our constituents voice committee, they are actively involved with advocacy programs and initiatives that will assist us in making sure that our members stay involved and engaged. So I'm gonna cut it short right there.
Speaker 1
Are there any other any questions for Michelle? All right. Go ahead and
Unknown Speaker
exit sooner
Unknown Speaker
that the only difference
Speaker 1
Yeah, you gotta need the mic. was speaking back there. Oh, by.
Speaker 13
The call center is like the front door and after they're enrolled in services, if there's any questions or issues or problems, then they'll go through customer service. Customer service kind of helps with the appeals and grievances, helping to coordinate like recipient rights complaints, but when they call in to access, they're getting a screening to see if they're eligible for services.
Speaker 16
And and the other part of is there this is just a small segment, we also do family subsidy support subsidy in some other areas of customer service. Okay, great. Thank you.
Speaker 1
Thank you. Any further questions? All right. Thank you. We will receive and file your report and we also are receiving and filing the Children's Services report. All right. The next one is integrated health.
Unknown Speaker
I found the numbers.
Speaker 1
Yeah. Yeah. Did you hear that you got a compliment? Good job on the numbers.
Speaker 17
Good 
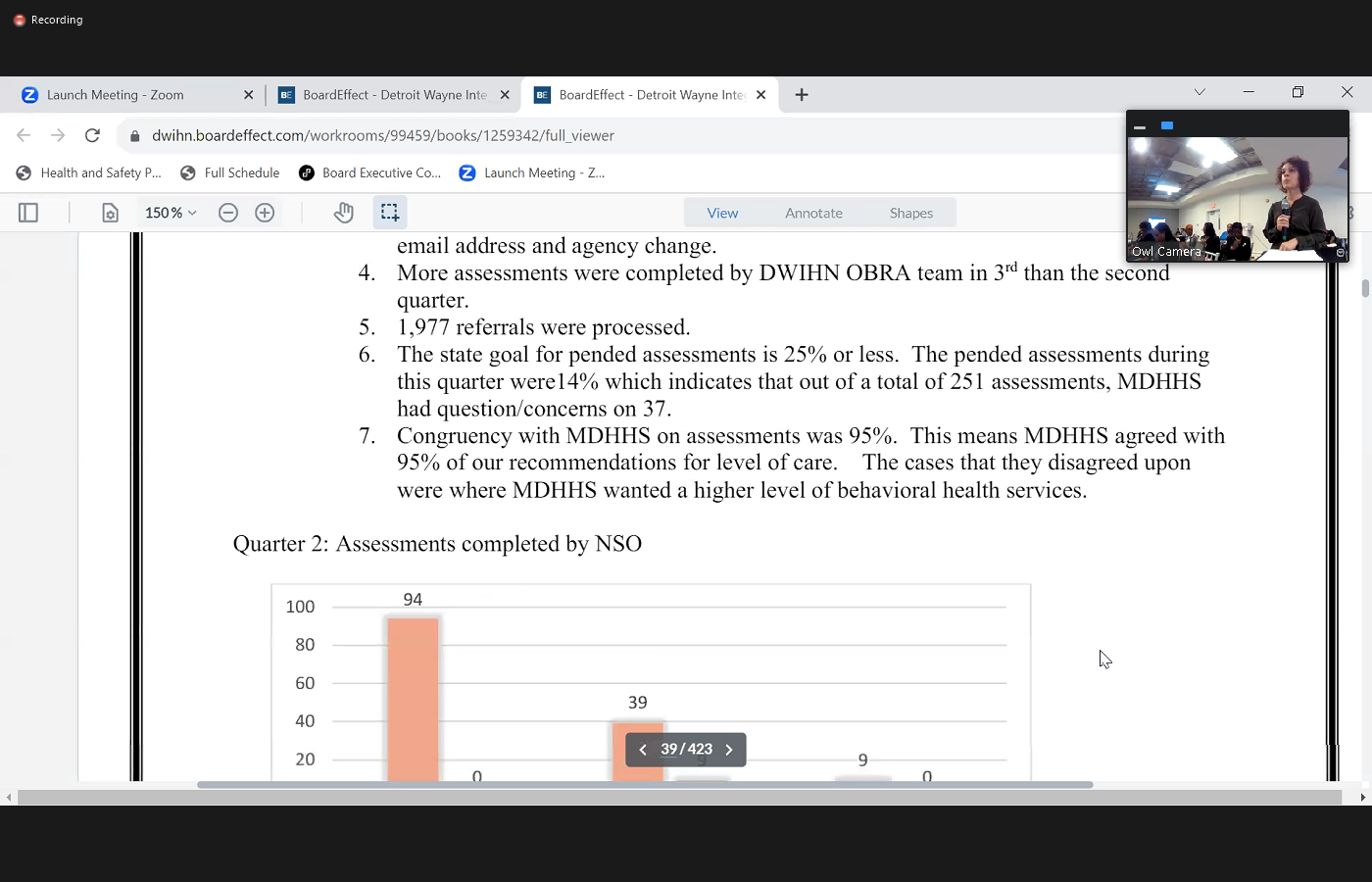 afternoon, Vicki pullets hausky, Director of integrated care. I will make this short. As we all know we took back the contract for obrah which was in the third quarter of this year. So just a little bit of statistics and how we're been doing. We'd had 1977 referrals in that first quarter that were processed. We completed 251 assessments. All those assessments have to go to the state and the state makes the final determination on the recommendations. Whether it's a nursing home placement, or what other services do they need. So on our pens, which means they had a question about an assessment, we had only 37 out of that 251 The state had questions on the second area that we look at, to make sure that we're doing a good job as congruency which means where are where our recommendations appropriate, and did the state agree with our recommendations? And that was at 95%. And our goal is to say 95% or higher. We doubled the number actually over doubled the number of assessments done on third quarter from second quarter. One areas that we are looking at right now. So we have what's called a queue
afternoon, Vicki pullets hausky, Director of integrated care. I will make this short. As we all know we took back the contract for obrah which was in the third quarter of this year. So just a little bit of statistics and how we're been doing. We'd had 1977 referrals in that first quarter that were processed. We completed 251 assessments. All those assessments have to go to the state and the state makes the final determination on the recommendations. Whether it's a nursing home placement, or what other services do they need. So on our pens, which means they had a question about an assessment, we had only 37 out of that 251 The state had questions on the second area that we look at, to make sure that we're doing a good job as congruency which means where are where our recommendations appropriate, and did the state agree with our recommendations? And that was at 95%. And our goal is to say 95% or higher. We doubled the number actually over doubled the number of assessments done on third quarter from second quarter. One areas that we are looking at right now. So we have what's called a queue 
 where the referrals come in at we have a four day queue which means they are in the hospital currently, and need an assessment done within four days to make sure do they need to get a nursing home placement or a different type of placement. We are at 100% with meeting that four day queue. The second one is the 14 day queue when we took over the contract. There were 300 assessments in there. We get about 150 assessments a month on that queue. So we all met executive leadership, finance, HR, we all met and we are going to look at contingent staff because that doesn't add to the final budget. And we can track that to see how many contingent staff and we should have that 300 Got down within the next three months with with contingent staff. Any questions on that? No. Okay, um, next one I'll go into is HEDIS measures I will just focus on two today. So f u h which is follow up after hospitalization, which means they need to be seen by a clinician within 30 days of discharge of that hospitalization. We now have our HEDIS scorecard so we can track that. The state tracks it, but there's a six to eight month lag so not in your real time. Ours is a 90 day lag. And so right now we are about 15% lower than we should be for adults and about 10% lower than we should be for children. We're meeting with all the providers so MCO access IHC quality, we're all in that meeting meeting with them, you know asking the providers What are they doing? What's their plan? How are they going to solve this problem? So we met with 23 providers in quarter three.
where the referrals come in at we have a four day queue which means they are in the hospital currently, and need an assessment done within four days to make sure do they need to get a nursing home placement or a different type of placement. We are at 100% with meeting that four day queue. The second one is the 14 day queue when we took over the contract. There were 300 assessments in there. We get about 150 assessments a month on that queue. So we all met executive leadership, finance, HR, we all met and we are going to look at contingent staff because that doesn't add to the final budget. And we can track that to see how many contingent staff and we should have that 300 Got down within the next three months with with contingent staff. Any questions on that? No. Okay, um, next one I'll go into is HEDIS measures I will just focus on two today. So f u h which is follow up after hospitalization, which means they need to be seen by a clinician within 30 days of discharge of that hospitalization. We now have our HEDIS scorecard so we can track that. The state tracks it, but there's a six to eight month lag so not in your real time. Ours is a 90 day lag. And so right now we are about 15% lower than we should be for adults and about 10% lower than we should be for children. We're meeting with all the providers so MCO access IHC quality, we're all in that meeting meeting with them, you know asking the providers What are they doing? What's their plan? How are they going to solve this problem? So we met with 23 providers in quarter three.  So the second one that's really important is fu A which is follow up after emergency room visit for alcohol or other drugs. Historically, D wind has been less than 20% than that. So the SU D department and IHC we got together to discuss how to do that. And as of quarter three, we are over 40% Now, so that's really good. We are in line with everyone else. In Michigan. And third one I'll talk about is our complex case management program. Who do see members it's a short term 120 Day program we had 12 new cases opened in third quarter. Nine cases were closed seven of those met all of their glow their goals. We have 73 presentations to the community. We we get a low number of satisfaction surveys so we worked with the IT department so we now can tax those satisfaction surveys. So we are getting a little bit more back. One other big thing with complex case management for such a small program is a very large part of NCQA. So we have been really, really working on that we're doing mock audits, monthly charts of all our paperwork, to make sure that we're meeting all the criteria for NCQA. So that is the end of my report.
So the second one that's really important is fu A which is follow up after emergency room visit for alcohol or other drugs. Historically, D wind has been less than 20% than that. So the SU D department and IHC we got together to discuss how to do that. And as of quarter three, we are over 40% Now, so that's really good. We are in line with everyone else. In Michigan. And third one I'll talk about is our complex case management program. Who do see members it's a short term 120 Day program we had 12 new cases opened in third quarter. Nine cases were closed seven of those met all of their glow their goals. We have 73 presentations to the community. We we get a low number of satisfaction surveys so we worked with the IT department so we now can tax those satisfaction surveys. So we are getting a little bit more back. One other big thing with complex case management for such a small program is a very large part of NCQA. So we have been really, really working on that we're doing mock audits, monthly charts of all our paperwork, to make sure that we're meeting all the criteria for NCQA. So that is the end of my report.
+3
afternoon, Vicki pullets hausky, Director of integrated care. I will make this short. As we all know we took back the contract for obrah which was in the third quarter of this year. So just a little bit of statistics and how we're been doing. We'd had 1977 referrals in that first quarter that were processed. We completed 251 assessments. All those assessments have to go to the state and the state makes the final determination on the recommendations. Whether it's a nursing home placement, or what other services do they need. So on our pens, which means they had a question about an assessment, we had only 37 out of that 251 The state had questions on the second area that we look at, to make sure that we're doing a good job as congruency which means where are where our recommendations appropriate, and did the state agree with our recommendations? And that was at 95%. And our goal is to say 95% or higher. We doubled the number actually over doubled the number of assessments done on third quarter from second quarter. One areas that we are looking at right now. So we have what's called a queue 
+2
where the referrals come in at we have a four day queue which means they are in the hospital currently, and need an assessment done within four days to make sure do they need to get a nursing home placement or a different type of placement. We are at 100% with meeting that four day queue. The second one is the 14 day queue when we took over the contract. There were 300 assessments in there. We get about 150 assessments a month on that queue. So we all met executive leadership, finance, HR, we all met and we are going to look at contingent staff because that doesn't add to the final budget. And we can track that to see how many contingent staff and we should have that 300 Got down within the next three months with with contingent staff. Any questions on that? No. Okay, um, next one I'll go into is HEDIS measures I will just focus on two today. So f u h which is follow up after hospitalization, which means they need to be seen by a clinician within 30 days of discharge of that hospitalization. We now have our HEDIS scorecard so we can track that. The state tracks it, but there's a six to eight month lag so not in your real time. Ours is a 90 day lag. And so right now we are about 15% lower than we should be for adults and about 10% lower than we should be for children. We're meeting with all the providers so MCO access IHC quality, we're all in that meeting meeting with them, you know asking the providers What are they doing? What's their plan? How are they going to solve this problem? So we met with 23 providers in quarter three. +1
So the second one that's really important is fu A which is follow up after emergency room visit for alcohol or other drugs. Historically, D wind has been less than 20% than that. So the SU D department and IHC we got together to discuss how to do that. And as of quarter three, we are over 40% Now, so that's really good. We are in line with everyone else. In Michigan. And third one I'll talk about is our complex case management program. Who do see members it's a short term 120 Day program we had 12 new cases opened in third quarter. Nine cases were closed seven of those met all of their glow their goals. We have 73 presentations to the community. We we get a low number of satisfaction surveys so we worked with the IT department so we now can tax those satisfaction surveys. So we are getting a little bit more back. One other big thing with complex case management for such a small program is a very large part of NCQA. So we have been really, really working on that we're doing mock audits, monthly charts of all our paperwork, to make sure that we're meeting all the criteria for NCQA. So that is the end of my report. Unknown Speaker
Then close
Speaker 9
the gap regarding the HEDIS get scores and the fu H the follow up that's done. Is it in in person follow up or are you also counting telemedicine follow up?
Unknown Speaker
We are including telehealth Yes. Yep.
Speaker 9
Do they continue to do telehealth going forward or is that just a way to meet this measure?
Speaker 17
They can continue to do to do telehealth moving forward. There are some stipulations and some guidelines on that but has to be in the person's treatment plan in the number of those that can't just only do telehealth to meet to meet that score, they need to be seen face to face in a certain amount of time. Good.
Speaker 9
They're really big question marks about the effectiveness of telemedicine with people who are severely ill defined hospitalized or certainly do exactly. Also, how do you track whether they follow up and continue with that first person follow up meeting? Someone is discharged they're seen by a provider 10 days later, but are they then seen by that same provider going forward for the next three 612 months? Or is it just different people? And again, we're just meeting a measure point
Speaker 17
within our he a scorecard. We can't track that but we can track that so I can look at that. With it of the people hospitalized because we're sending all the data that gets put into the scorecard. So we can track that. I am working with adults initiatives right now because that's where most of our work needs to be. And they have specific staff assigned to specific providers. And we will there are three new staff so I'm training them this month and the scorecard how to pull the data how to look at the data, and then we can pull reports or make reports to make sure those follow up and we can track like like you said, is it just like are they just meeting like a one time therapist and then never been seen? Again? Right kind of thing? Yeah, it's
Speaker 9
attracted us with the same therapist, right? Because you have to develop that relationship, especially in psychiatry. And if that's never established, we're really not making a difference right.
Speaker 17
And you should see with a decrease of hospitalizations usage should see an increase of outpatient. You know, and we actually were discussing that with one of the health plans the other day of how that goes because they're like, well, we should see a decrease in both and I'm like, No, you should see a decrease in hospitalization increase in outpatient, whether that's case management therapy or psychiatry or all of the
Speaker 9
above and follow the pharmacy to because oftentimes hospitalizations are because they don't have access to are compliant with medications.
Speaker 17
Yep. And we're working right now within our platform to actually get the pharmacy data in there as timely as we can work on some Covina issues.
Speaker 1
Without regard. Would you like to see us at the next quarterly report, perhaps to do a snapshot of those issues that you brought up, but she can give us some feedback. So I'll export the report. Okay. Yeah. All right. Thank you. Thank you. Any further questions? All right. Thank you. We will receive and file the integrated care report now assigned for the disparity of racial disparities. I would ask I think we've looked at that we know that there's a disparity clearly. Tell us a little bit about what's been done to to correct
Unknown Speaker
the disparity. Yes.
Speaker 14
Thank 
 you again. Good afternoon, Madam Chair, distinguished board members, a perceiver, Director of Quality Improvement. You right I will be presenting on the hospital discharge follow ratio disparity. I will try to be brief. I do want to focus on why this PIP is important and to what we are doing pacifically to reduce the racial disparity that exists in our network. I think it's important first to highlight that in 2022 the health service advisory group which is a sec, who is contracted with MDHHS as an external auditor directed all the PHPs in the state to create a three year PIP on racial disparity in the network. And based on our review and our analysis of our data, we found a disparity gap between the percentage of African Americans compared to white members who receive follow up care within seven days of discharge from a hospital. Can we go to the next slide please? The summary of that timeline is that the PIP valid that the PIP was submitted to the ASAP for validation on July 25 And then we resubmitted it because there was some revisions that we need to make we needed to make and it
you again. Good afternoon, Madam Chair, distinguished board members, a perceiver, Director of Quality Improvement. You right I will be presenting on the hospital discharge follow ratio disparity. I will try to be brief. I do want to focus on why this PIP is important and to what we are doing pacifically to reduce the racial disparity that exists in our network. I think it's important first to highlight that in 2022 the health service advisory group which is a sec, who is contracted with MDHHS as an external auditor directed all the PHPs in the state to create a three year PIP on racial disparity in the network. And based on our review and our analysis of our data, we found a disparity gap between the percentage of African Americans compared to white members who receive follow up care within seven days of discharge from a hospital. Can we go to the next slide please? The summary of that timeline is that the PIP valid that the PIP was submitted to the ASAP for validation on July 25 And then we resubmitted it because there was some revisions that we need to make we needed to make and it  was accepted by a sec on November in November, and we receive 100% on our baseline data report. And that was based on the methodology that we're going to use to measure this and also the initial interventions that we identified that we were going to use the next slide please. The next slide just reflect the baseline data that we collected and we submitted to the state for approval. Okay, the next slide please. Following the analysis of the baseline, these are some of the general interventions that we identify that we were going to do. We want to have monthly meetings with the Chris to educate them and to share the data with them. Secondly, we will also going to provide them access to our portal portal so they can review their data at any time and they can self monitor their own data. Third, we also educated their medical directors at their agency for them to understand the gap that we have within our next network as it relates to disparity and for them to review the data. And then we also work with our finance department to develop a value based performance and setup that was
was accepted by a sec on November in November, and we receive 100% on our baseline data report. And that was based on the methodology that we're going to use to measure this and also the initial interventions that we identified that we were going to use the next slide please. The next slide just reflect the baseline data that we collected and we submitted to the state for approval. Okay, the next slide please. Following the analysis of the baseline, these are some of the general interventions that we identify that we were going to do. We want to have monthly meetings with the Chris to educate them and to share the data with them. Secondly, we will also going to provide them access to our portal portal so they can review their data at any time and they can self monitor their own data. Third, we also educated their medical directors at their agency for them to understand the gap that we have within our next network as it relates to disparity and for them to review the data. And then we also work with our finance department to develop a value based performance and setup that was  provided to those compliant providers who was meeting the the seven day follow up. Where are we now? Okay, this is our luminary day of where we are now. The preliminary data right now reveals that we had a 9% disparity gap within our network. Right now we are reviewing our data monthly. We did see that in July that it revealed a disparity gap of 5.63%. So it does tell us that is going down that some of the interventions are working. The data is also telling us that while the seven day compliance for African American members were 32.94%. The data also demonstrated that African Americans that we're not seeing within the seven days we're eventually seen and an overall compliance rate of 59.82%. So that means 648 of our members followed up with their provider outside of the seven days. So that tells us that our providers are engaging with the members re engaging with them sending Texas sending letters. So that was encouraging as well. So from the preliminary data, we develop more targeted interventions that we're going to do because again, we're not satisfied as to where we are. Right now. IHC has been reaching
provided to those compliant providers who was meeting the the seven day follow up. Where are we now? Okay, this is our luminary day of where we are now. The preliminary data right now reveals that we had a 9% disparity gap within our network. Right now we are reviewing our data monthly. We did see that in July that it revealed a disparity gap of 5.63%. So it does tell us that is going down that some of the interventions are working. The data is also telling us that while the seven day compliance for African American members were 32.94%. The data also demonstrated that African Americans that we're not seeing within the seven days we're eventually seen and an overall compliance rate of 59.82%. So that means 648 of our members followed up with their provider outside of the seven days. So that tells us that our providers are engaging with the members re engaging with them sending Texas sending letters. So that was encouraging as well. So from the preliminary data, we develop more targeted interventions that we're going to do because again, we're not satisfied as to where we are. Right now. IHC has been reaching  out to those members that have been hospitalized, who has been discharged within two or three days. They are assisting now with coordination of assisting them excuse me with care coordination meaning that asking them do you need assistance, educating them on the importance of your follow up appointment? We also have contracted with to vendors who are providing I'm sorry, who I have sorry, who are providing who are addressing and assisting us with transit, any transportation barriers that our members are having. We also are working with our customer service department, our member experience department in coordination with quality and working on collaboration of a survey. And we surveyed that will excuse me, that will survey those members who did not make their appointment to see why you're not making your appointment. What are some of the things that we can do? Is it because of the location? Is it because of the provider? Why you're not making your appointment? So we're going to drill down and get that data as well. We're going to continue to meet with our crisp providers, but we're going to target it those providers that have a high disparity rate. We're going to target those providers. And we're going to continue to meet with the power providers but we're just targeting those providers that have a high disparity rate and work with them to see what are you doing in your organization? What are the was some of the barriers you having? How can we assess how can the witnesses lastly our quality team through their performance monitoring. They have been focusing on reviewing sample cases of members who did not make their appointment to ensure that the providers are re engaging them that even though you did not make your appointment that we are reaching out to you trying to get you in for an appointment we are going to continue to meet our quality team are going to continue to meet on a bi weekly on excuse me on a bite every two weeks to discuss how we're doing with our interventions, how we're going with our interventions. We also going to continue to meet with the liaison the hospital liaison because we want to ensure that there are clear coordination of care with the hospital and the crisp providers so we can make sure that they know that that is that that information is trickling down as well. And then lastly, I'm not running out of time. No less than monopoly. I will, you know, bring back to the PCC committee to let you guys know how we're doing in terms of our our interventions. And I will pause there and take questions. I'm sorry I was trying harder Yes.
out to those members that have been hospitalized, who has been discharged within two or three days. They are assisting now with coordination of assisting them excuse me with care coordination meaning that asking them do you need assistance, educating them on the importance of your follow up appointment? We also have contracted with to vendors who are providing I'm sorry, who I have sorry, who are providing who are addressing and assisting us with transit, any transportation barriers that our members are having. We also are working with our customer service department, our member experience department in coordination with quality and working on collaboration of a survey. And we surveyed that will excuse me, that will survey those members who did not make their appointment to see why you're not making your appointment. What are some of the things that we can do? Is it because of the location? Is it because of the provider? Why you're not making your appointment? So we're going to drill down and get that data as well. We're going to continue to meet with our crisp providers, but we're going to target it those providers that have a high disparity rate. We're going to target those providers. And we're going to continue to meet with the power providers but we're just targeting those providers that have a high disparity rate and work with them to see what are you doing in your organization? What are the was some of the barriers you having? How can we assess how can the witnesses lastly our quality team through their performance monitoring. They have been focusing on reviewing sample cases of members who did not make their appointment to ensure that the providers are re engaging them that even though you did not make your appointment that we are reaching out to you trying to get you in for an appointment we are going to continue to meet our quality team are going to continue to meet on a bi weekly on excuse me on a bite every two weeks to discuss how we're doing with our interventions, how we're going with our interventions. We also going to continue to meet with the liaison the hospital liaison because we want to ensure that there are clear coordination of care with the hospital and the crisp providers so we can make sure that they know that that is that that information is trickling down as well. And then lastly, I'm not running out of time. No less than monopoly. I will, you know, bring back to the PCC committee to let you guys know how we're doing in terms of our our interventions. And I will pause there and take questions. I'm sorry I was trying harder Yes.
+2
you again. Good afternoon, Madam Chair, distinguished board members, a perceiver, Director of Quality Improvement. You right I will be presenting on the hospital discharge follow ratio disparity. I will try to be brief. I do want to focus on why this PIP is important and to what we are doing pacifically to reduce the racial disparity that exists in our network. I think it's important first to highlight that in 2022 the health service advisory group which is a sec, who is contracted with MDHHS as an external auditor directed all the PHPs in the state to create a three year PIP on racial disparity in the network. And based on our review and our analysis of our data, we found a disparity gap between the percentage of African Americans compared to white members who receive follow up care within seven days of discharge from a hospital. Can we go to the next slide please? The summary of that timeline is that the PIP valid that the PIP was submitted to the ASAP for validation on July 25 And then we resubmitted it because there was some revisions that we need to make we needed to make and it +1
was accepted by a sec on November in November, and we receive 100% on our baseline data report. And that was based on the methodology that we're going to use to measure this and also the initial interventions that we identified that we were going to use the next slide please. The next slide just reflect the baseline data that we collected and we submitted to the state for approval. Okay, the next slide please. Following the analysis of the baseline, these are some of the general interventions that we identify that we were going to do. We want to have monthly meetings with the Chris to educate them and to share the data with them. Secondly, we will also going to provide them access to our portal portal so they can review their data at any time and they can self monitor their own data. Third, we also educated their medical directors at their agency for them to understand the gap that we have within our next network as it relates to disparity and for them to review the data. And then we also work with our finance department to develop a value based performance and setup that was +1
provided to those compliant providers who was meeting the the seven day follow up. Where are we now? Okay, this is our luminary day of where we are now. The preliminary data right now reveals that we had a 9% disparity gap within our network. Right now we are reviewing our data monthly. We did see that in July that it revealed a disparity gap of 5.63%. So it does tell us that is going down that some of the interventions are working. The data is also telling us that while the seven day compliance for African American members were 32.94%. The data also demonstrated that African Americans that we're not seeing within the seven days we're eventually seen and an overall compliance rate of 59.82%. So that means 648 of our members followed up with their provider outside of the seven days. So that tells us that our providers are engaging with the members re engaging with them sending Texas sending letters. So that was encouraging as well. So from the preliminary data, we develop more targeted interventions that we're going to do because again, we're not satisfied as to where we are. Right now. IHC has been reaching +1
out to those members that have been hospitalized, who has been discharged within two or three days. They are assisting now with coordination of assisting them excuse me with care coordination meaning that asking them do you need assistance, educating them on the importance of your follow up appointment? We also have contracted with to vendors who are providing I'm sorry, who I have sorry, who are providing who are addressing and assisting us with transit, any transportation barriers that our members are having. We also are working with our customer service department, our member experience department in coordination with quality and working on collaboration of a survey. And we surveyed that will excuse me, that will survey those members who did not make their appointment to see why you're not making your appointment. What are some of the things that we can do? Is it because of the location? Is it because of the provider? Why you're not making your appointment? So we're going to drill down and get that data as well. We're going to continue to meet with our crisp providers, but we're going to target it those providers that have a high disparity rate. We're going to target those providers. And we're going to continue to meet with the power providers but we're just targeting those providers that have a high disparity rate and work with them to see what are you doing in your organization? What are the was some of the barriers you having? How can we assess how can the witnesses lastly our quality team through their performance monitoring. They have been focusing on reviewing sample cases of members who did not make their appointment to ensure that the providers are re engaging them that even though you did not make your appointment that we are reaching out to you trying to get you in for an appointment we are going to continue to meet our quality team are going to continue to meet on a bi weekly on excuse me on a bite every two weeks to discuss how we're doing with our interventions, how we're going with our interventions. We also going to continue to meet with the liaison the hospital liaison because we want to ensure that there are clear coordination of care with the hospital and the crisp providers so we can make sure that they know that that is that that information is trickling down as well. And then lastly, I'm not running out of time. No less than monopoly. I will, you know, bring back to the PCC committee to let you guys know how we're doing in terms of our our interventions. And I will pause there and take questions. I'm sorry I was trying harder Yes. Speaker 9
So to achieve 100% keeping appointments, if you solve that, you will run the world but with that in mind, have you considered things happen that prevent people from making appointments? Minute by minute? Yes, my intention is to go tomorrow at 9am. But something happens and I think in certain subsets of populations the ability to have chaos is higher. So have you ever thought about just telling the discharge patients please show up within the next seven days whenever you walk in we'll see you
Speaker 14
know we have not I don't think that language have ever been conveyed. To our members. But there's something that we can take back because as I stated we are meeting with the Chris, we are meeting with the liaison and that's something that we can share with them. I'm sorry, Doctor to him. Did you want to I'm sorry. I'm sorry. Yeah, that's something that we can take back. Like I said we are meeting with them on a monthly basis. And that's something that I can share with them. Because we are also meeting with the liaisons from the hospital. So that's something that we can share with them. Yes.
Speaker 9
And then secondly, I like that you're providing transportation because that's often a hurdle. But again, if I have that 9am appointment and mariners in is coming to get me at nine and I can't make it, but I could have made it at 12 Is there any follow up or Mariners and come back and get me or have you thought about giving them an Uber card, and whenever they can make it they can schedule their own transportation.
Speaker 14
That's a very, very excellent thought. And that's something that I don't think we consider it but there's something that I can take back to the team and that's something that we can consider implementing. Yes, that's a very good, very good,
Unknown Speaker
Dr. Moody and then we gotta keep going. Yes. I thought that was that took the heat. I'm sorry, I misspoke.
Speaker 5
I think April answered the walk in hours. Right now our providers don't have walk in hours, but that's something that we have been bringing up to them.
Unknown Speaker
Thank you. All right, Mr. Parker. Did you have
Speaker 7
you ever done focus groups are those people that do not show up for the appointments to see what some I know you did individual surveys, sometimes the focus groups is opportunity to focus on why they did not show up.
Speaker 14
And that's something that we can Yeah, we can consider doing one yes, we have not done that. Yes. Thank you. Thank you for those. Thank
Speaker 1
you. Yes, we're just focusing on the highlights. Okay, thank you. That's very important work so we're not minimizing the important understand that yes, thank you. All right, we will receive and file this report. All right, I'll miss moody. It's we have you here please just a highlight because we got about I hate that. I hate to dump that on you but we've got a lot of a board action to consider. So and I like her to be done by four. Okay. Okay. Thank you.
Unknown Speaker
Thank you Madam Chair and board members.
Unknown Speaker
So by four by three.
Unknown Speaker
If we have to before I could go a little longer. Thank you for
Speaker 15
good afternoon, Melissa moody VP of Clinical Operations. You have my report in the packet since I'm gonna highlight a few areas. The first is our habilitative support waiver. We have been working very diligently as an organization and a network to increase our enrollment in this waiver program, that the state enrollment requirement is an expectation is 95%. And we had fallen below that 95% For for some time, trying to get people enrolled and this is an enhanced benefit for members. So it's a really great program to be in. So back in March, we put it step forth 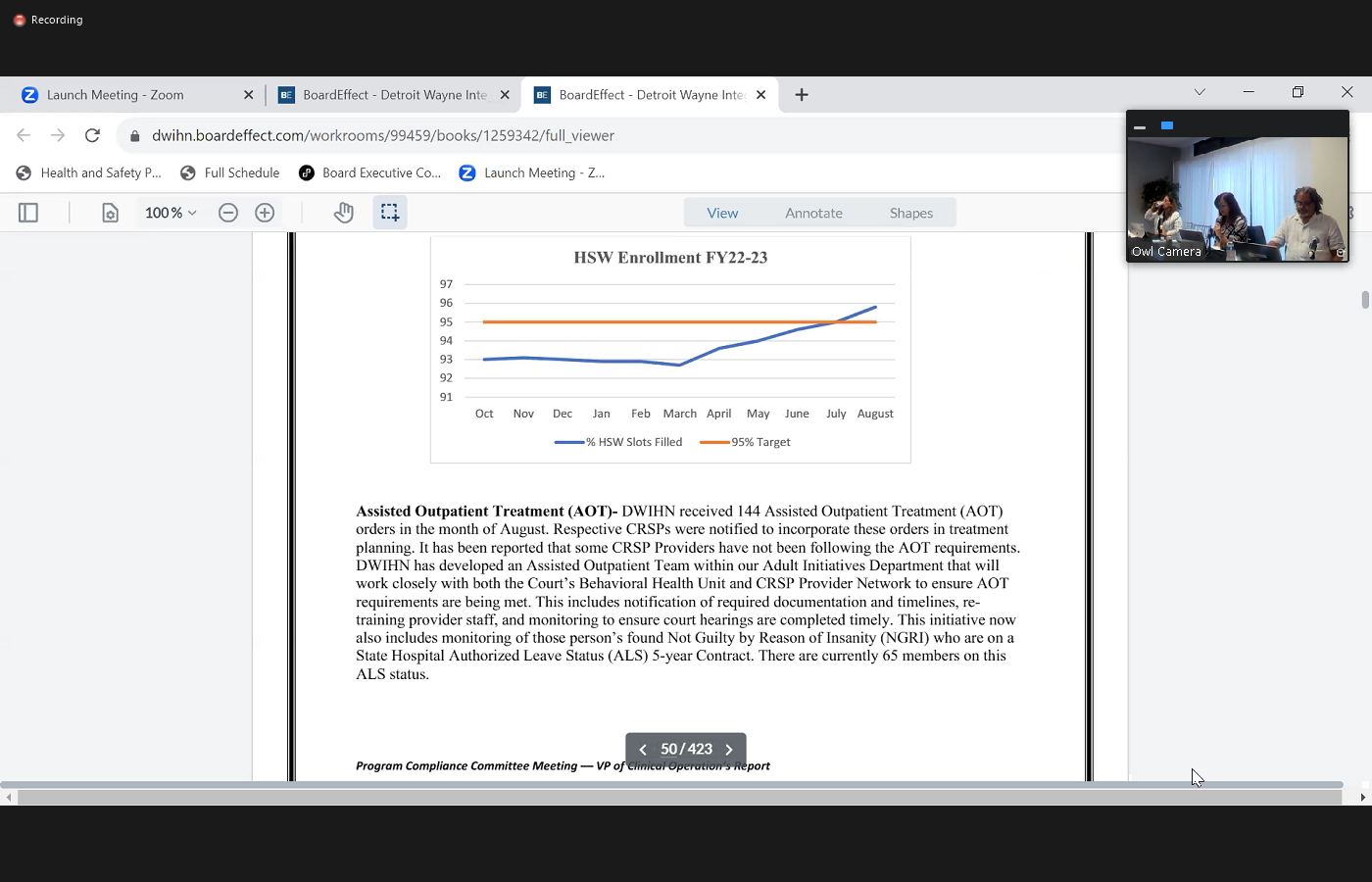
 and internal corrective plan that we put into place with a variety of different steps to work with our provider network, both in internally and externally to get those numbers of enrollments increased. And as you can see, we've, we've finally hit that 95% benchmark in July, and we continue to increase in those enrollments. So it took us about four months of this corrective plan, but we have met the target and we have continued to go up. So we're very optimistic about that. process as well. And we're going to continue to have those efforts going forward as well. Another area is just to highlight is our substance use services. We heard there's some data here regarding our discharges from withdrawal management. detox and the number of persons that are following up within seven days. And as you can see, July we had 92.69% follow up and in August, it's 96.3. So we're continuing to see that follow up as well. So Sud services is really doing a good job and engagement and getting persons into services that support them. And then additionally, or CCBHC I have no great news to share, or no recent news. We have
and internal corrective plan that we put into place with a variety of different steps to work with our provider network, both in internally and externally to get those numbers of enrollments increased. And as you can see, we've, we've finally hit that 95% benchmark in July, and we continue to increase in those enrollments. So it took us about four months of this corrective plan, but we have met the target and we have continued to go up. So we're very optimistic about that. process as well. And we're going to continue to have those efforts going forward as well. Another area is just to highlight is our substance use services. We heard there's some data here regarding our discharges from withdrawal management. detox and the number of persons that are following up within seven days. And as you can see, July we had 92.69% follow up and in August, it's 96.3. So we're continuing to see that follow up as well. So Sud services is really doing a good job and engagement and getting persons into services that support them. And then additionally, or CCBHC I have no great news to share, or no recent news. We have 
 not heard anything from our SAMSA grant application yet. We were informed we probably should have heard a couple of weeks ago, but no one has gotten any results. So we're still waiting to hear about that application. The state demonstration continues to move forward with adding more providers to that demonstration in our region. They have added five providers in our network that are now going to be CCBHC state demonstration sites. So that's going to be starting on October 1. So we're working with those providers to get them up and ready while we continue to move ourselves forward in that clinical direction. So at this time, we are working and getting focused on getting ourselves ready for certification and providing direct clinical services as well. And then I have listed out just for your you review we have done a multitude of RFPs or an RFIs to make sure we have provider capacity in our network. So we can make make sure people have access to those needed appointments as well. And then finally, something not listed in the report. Just want to let you know we did launch our peers to higher education partnership with Wayne State University, which focuses on enhancing the behavioral health workforce by creating a pathway for peer specialists to become licensed social workers and addiction counselors. So we're very excited about this initiative that started this fall. And that concludes my report. I'm available for any questions.
not heard anything from our SAMSA grant application yet. We were informed we probably should have heard a couple of weeks ago, but no one has gotten any results. So we're still waiting to hear about that application. The state demonstration continues to move forward with adding more providers to that demonstration in our region. They have added five providers in our network that are now going to be CCBHC state demonstration sites. So that's going to be starting on October 1. So we're working with those providers to get them up and ready while we continue to move ourselves forward in that clinical direction. So at this time, we are working and getting focused on getting ourselves ready for certification and providing direct clinical services as well. And then I have listed out just for your you review we have done a multitude of RFPs or an RFIs to make sure we have provider capacity in our network. So we can make make sure people have access to those needed appointments as well. And then finally, something not listed in the report. Just want to let you know we did launch our peers to higher education partnership with Wayne State University, which focuses on enhancing the behavioral health workforce by creating a pathway for peer specialists to become licensed social workers and addiction counselors. So we're very excited about this initiative that started this fall. And that concludes my report. I'm available for any questions.
+2
and internal corrective plan that we put into place with a variety of different steps to work with our provider network, both in internally and externally to get those numbers of enrollments increased. And as you can see, we've, we've finally hit that 95% benchmark in July, and we continue to increase in those enrollments. So it took us about four months of this corrective plan, but we have met the target and we have continued to go up. So we're very optimistic about that. process as well. And we're going to continue to have those efforts going forward as well. Another area is just to highlight is our substance use services. We heard there's some data here regarding our discharges from withdrawal management. detox and the number of persons that are following up within seven days. And as you can see, July we had 92.69% follow up and in August, it's 96.3. So we're continuing to see that follow up as well. So Sud services is really doing a good job and engagement and getting persons into services that support them. And then additionally, or CCBHC I have no great news to share, or no recent news. We have +2
not heard anything from our SAMSA grant application yet. We were informed we probably should have heard a couple of weeks ago, but no one has gotten any results. So we're still waiting to hear about that application. The state demonstration continues to move forward with adding more providers to that demonstration in our region. They have added five providers in our network that are now going to be CCBHC state demonstration sites. So that's going to be starting on October 1. So we're working with those providers to get them up and ready while we continue to move ourselves forward in that clinical direction. So at this time, we are working and getting focused on getting ourselves ready for certification and providing direct clinical services as well. And then I have listed out just for your you review we have done a multitude of RFPs or an RFIs to make sure we have provider capacity in our network. So we can make make sure people have access to those needed appointments as well. And then finally, something not listed in the report. Just want to let you know we did launch our peers to higher education partnership with Wayne State University, which focuses on enhancing the behavioral health workforce by creating a pathway for peer specialists to become licensed social workers and addiction counselors. So we're very excited about this initiative that started this fall. And that concludes my report. I'm available for any questions. Unknown Speaker
Any questions for Melissa moody,
Speaker 6
if I may. I was just gonna ask a question in terms of the JD funding. Please comment on that.
Speaker 15
The the facility? Yes. Okay. Yes. So currently, you know, we talked a lot about the jewel juvenile restorative program at teen wellness it that they're doing outpatient, and we had been working with the state to figure out how funds could be provided to provide in JTF services so they would get services within the facility that Dickerson facility. So we had numerous contacts with the state. And we did find out there was state funding available that the counties could apply for, or the county I should say Wayne County could apply for they did apply for those funds. And they are providing when are going into a contract with Team wellness to provide in house JDF clinical services with those funds.
Speaker 1
That's great. Thank you. All right. Thank you for that clarification. Thank you. Any questions? All right. Thank you, Miss moody will receive and file your report. We're now at board action. So we've got quite a few of them. So we'll start in then with the unfinished business board action 2108 healthcare effectiveness data information set this is the HEDIS Yes. Yes. If I may, Mr. Adams is joining the call. He's been on the call the entire time. So I just wanted to acknowledge Okay, thank you. Thank you. All right. There any I assume everybody got these. This is not the one that was added today. So any questions about this board item 2109. Go ahead. I don't know how to say your last name. Well it Caskey Allah kowski Okay, thank you.
Speaker 17
Board  action 21 dash O eight, R two. So this is we are exercising a two year a to one year extensions with vital data technologies for our HEDIS platform. Currently we have 15 HEDIS measures, we are going to be adding 27 additional measures for the ow hh BHH and CCBHC. So the amount is not to exceed 1,000,686 $564. That is an increase of 840,564 due to those added extra measures that we're going to be adding to it along with those measures they will be broken down by race to so we will be able to see those each measures by race.
action 21 dash O eight, R two. So this is we are exercising a two year a to one year extensions with vital data technologies for our HEDIS platform. Currently we have 15 HEDIS measures, we are going to be adding 27 additional measures for the ow hh BHH and CCBHC. So the amount is not to exceed 1,000,686 $564. That is an increase of 840,564 due to those added extra measures that we're going to be adding to it along with those measures they will be broken down by race to so we will be able to see those each measures by race.
+1
action 21 dash O eight, R two. So this is we are exercising a two year a to one year extensions with vital data technologies for our HEDIS platform. Currently we have 15 HEDIS measures, we are going to be adding 27 additional measures for the ow hh BHH and CCBHC. So the amount is not to exceed 1,000,686 $564. That is an increase of 840,564 due to those added extra measures that we're going to be adding to it along with those measures they will be broken down by race to so we will be able to see those each measures by race. Speaker 1
Question Move approval. Okay, that will always be moved in support it any further discussion? The no hands all in favor signify by saying aye. Aye. Any opposed? And the abstentions? All right. Thank you very much. Okay, we'll move on to the next board action. Miss Davis.
Speaker 18
Good afternoon, Jacqueline Davis Clinical Officer. This is board action 2320 Rs revised board action we're requesting approval for a one year extension in the amount not to exceed 335,500.
Speaker 1
All right. Go ahead. Miss Bullock. Did you have a question? Oh, I'm sorry. Any comments? Any questions? All right. We need a motion to approve it. This this move by Mr. Phillips? Is there support? Port by Miss Bullock in further discussion? Hearing none, all in favor signify by saying aye. Aye. Any opposed? Any abstentions? All right. Thank you. All right. The next one my health link. Demonstration Project missteps. Sorry, that's not me. Oh, that's not you. Oh, I'm sorry. This is a revised one. Yes.
Speaker 12
Yeah.  Where are you seeing Lluch VP of operations. The board action 2346 Division Two is in front of you. This is a matter of collaborative. We are adding $50,000 to add to provide add another Medicare provider for speech, occupational and physical therapies. This is again, as you know, is a pass through our health plans, reimburse those for the services providers. So this is just to augment the need that was there by expanding into that specific provider for those services.
Where are you seeing Lluch VP of operations. The board action 2346 Division Two is in front of you. This is a matter of collaborative. We are adding $50,000 to add to provide add another Medicare provider for speech, occupational and physical therapies. This is again, as you know, is a pass through our health plans, reimburse those for the services providers. So this is just to augment the need that was there by expanding into that specific provider for those services.
+1
Where are you seeing Lluch VP of operations. The board action 2346 Division Two is in front of you. This is a matter of collaborative. We are adding $50,000 to add to provide add another Medicare provider for speech, occupational and physical therapies. This is again, as you know, is a pass through our health plans, reimburse those for the services providers. So this is just to augment the need that was there by expanding into that specific provider for those services. Unknown Speaker
All right. Thank you. Is there a motion to approve?
Unknown Speaker
Move by Miss Bull if I may, if I may, Madam Chair.
Speaker 1
Well, I need to get a support support.
Speaker 3
I asked that Mr. Phillips please recuse himself for hearing for our health systems. Regarding the vote.
Unknown Speaker
Okay. Thank you.
Speaker 10
I'm under discussion. So I didn't make you aware of my conflict. Could you highlight if there is a conflict anywhere in any of this?
Unknown Speaker
I'll flag you who's coming.
Speaker 1
Thank you. All right, any further discussion on this? Moved and supported all in favor signify by saying aye. Aye. Any opposed? Any abstentions? one abstention. Mr. Phillips. All right. Thank you. Motion passed. We're now a new business. And we're looking at board action. 2401 that is Miss Smith.
Speaker 4
Thank  you, Cassandra. Phillips, Director children's initiatives presenting board action Toony four dash O one. This time we are actually combining all of our children's initiatives. MD HS grants together into one board action. So we are requesting for the contract. You're starting October one for $1,593,030. For all of the all of the grants, and the grants include the system of care block grant, the infant early childhood mental health consultation, Grant, infant and early childhood mental health consultation and home visiting grant. The infant and early childhood mental health consultation expansion grant and infant toddler Court program grant.
you, Cassandra. Phillips, Director children's initiatives presenting board action Toony four dash O one. This time we are actually combining all of our children's initiatives. MD HS grants together into one board action. So we are requesting for the contract. You're starting October one for $1,593,030. For all of the all of the grants, and the grants include the system of care block grant, the infant early childhood mental health consultation, Grant, infant and early childhood mental health consultation and home visiting grant. The infant and early childhood mental health consultation expansion grant and infant toddler Court program grant.
+1
you, Cassandra. Phillips, Director children's initiatives presenting board action Toony four dash O one. This time we are actually combining all of our children's initiatives. MD HS grants together into one board action. So we are requesting for the contract. You're starting October one for $1,593,030. For all of the all of the grants, and the grants include the system of care block grant, the infant early childhood mental health consultation, Grant, infant and early childhood mental health consultation and home visiting grant. The infant and early childhood mental health consultation expansion grant and infant toddler Court program grant. Speaker 1
Right there motion to approve. So moved. Moved by Dr. Carter. Is there support support by Miss Bullock any further discussion? The no hands all in favor signify by saying aye. Aye. Any opposed? Any abstentions? All right. Thank you. The motion carries. Next board action 2409.
Speaker 12
Madam 
 Chair, yeah, Penny swingler VP of operations. The 2409. Va is for Michigan Rehabilitation. Services. This was a continued program for this year, for a total amount of 443,005 65. This is an interagency with a matching program from Mrs in the amount of 1.1 million approximately being in total revenue for this important initiative that basically provide employment opportunities and, and training opportunities for members with IDD. And it is an extremely valuable resource for those individuals.
Chair, yeah, Penny swingler VP of operations. The 2409. Va is for Michigan Rehabilitation. Services. This was a continued program for this year, for a total amount of 443,005 65. This is an interagency with a matching program from Mrs in the amount of 1.1 million approximately being in total revenue for this important initiative that basically provide employment opportunities and, and training opportunities for members with IDD. And it is an extremely valuable resource for those individuals.
+2
Chair, yeah, Penny swingler VP of operations. The 2409. Va is for Michigan Rehabilitation. Services. This was a continued program for this year, for a total amount of 443,005 65. This is an interagency with a matching program from Mrs in the amount of 1.1 million approximately being in total revenue for this important initiative that basically provide employment opportunities and, and training opportunities for members with IDD. And it is an extremely valuable resource for those individuals. Speaker 1
I found it interesting that we had it since 1994. But in any case, go ahead Is there a support for this most for this support action? Like the motion to support? Motion to approve. So move? Moved by Mr. Commissioner camlock. Is there support? Support by Miss Bullock any further discussion? Hearing none, all in favor signify by saying aye. Aye. Any opposed? Any abstentions? Thank you. Okay, next board action. This is jail diversion. What action 2410
Speaker 19
Good afternoon. I'm Andrea Smith, Director of Innovation community engagement. And this board action is requesting support and approval of funds. For our police partnerships and diversion efforts with Grosse Pointe Police Department, extra Police Department, Team wellness, CNS healthcare, Central City integrated health and the Southgate veteran's treatment court. Right.
Speaker 1
Is there a motion to approve? Mr. Phillips, is there support support supported by Commissioner Kinloch any further discussion? I see no hands all in favor signify by saying aye. Aye. Any opposed? Any abstentions? All right. Thank you carries. All right board action. 2412. No, you go right ahead.
Speaker 20
Good  afternoon, Judy Davis, Sud director, board action 2412. We are asking to deliver Sud tribute services for fiscal year 24. Not to exceed the amount of $6,765,483 5 million is in black Rand and a million ism pa two funds and this also covers COVID-19 Women specialty service, our performance of state opioid response in media efforts.
afternoon, Judy Davis, Sud director, board action 2412. We are asking to deliver Sud tribute services for fiscal year 24. Not to exceed the amount of $6,765,483 5 million is in black Rand and a million ism pa two funds and this also covers COVID-19 Women specialty service, our performance of state opioid response in media efforts.
+1
afternoon, Judy Davis, Sud director, board action 2412. We are asking to deliver Sud tribute services for fiscal year 24. Not to exceed the amount of $6,765,483 5 million is in black Rand and a million ism pa two funds and this also covers COVID-19 Women specialty service, our performance of state opioid response in media efforts. Speaker 1
Their motion to approve move by Mr. Phillips and their support the port by Miss Bullock any further discussion?
Unknown Speaker
Let the record reflect I abstain.
Speaker 1
You're going to abstain why? Did it go down so much because the year previously it was quite a bit several million more.
Speaker 20
What actually we added a like a $2 million increase. Some of the numbers are not including this because it goes throughout image when system. These are numbers that is only built throughout FSR process. Like oh,
Speaker 21
God, I'm sorry, Madam Chair. Yes, it actually did go down because of the COVID grant we have received in fiscal 23. A significant amount of COVID funds that did not pan out come over is at the dollar value that it previously had. Come.
Unknown Speaker
All right. Thank you. I thought I saw that it went down. So
Speaker 20
it did today. Those COVID funds is just through the march. So is half of the year. All
Speaker 1
right. All right. Thank you for that clarification. All right. We're ready for a vote all in favor signify by saying Aye. Any opposed? Any abstentions? Abstain? Yeah. Commissioner Kinloch. All right board action 2413. Also su De.
Speaker 20
Su de is requesting to deliver su Dietrich prevention services for fiscal year 24 not to exceed the amount of 6,492,000 and this also includes for COVID-19, our state state opioid response and operant tobacco funds.
Unknown Speaker
Alright, great. Is there a motion to approve? Move by Miss Bullock is there support? This support support by Mr. Phillips? All right, any further discussion?
Speaker 1
The no hands all in favor signify by saying aye. Aye. Any opposed? Any abstentions? one abstention Commissioner Kembla Thank you. All right board action 2414 multicultural integration programs.
Speaker 19
Yes, ma'am. I'm Andrea Smith. Again, this board action will not exceed $784,540. This is Black grant funds to disperse. So it comes to do when we pass through to American Indian Health and Family Services Association of Chinese Americans. Community Health and Social Services and southwest counseling solutions. And the funds also support our veteran veteran navigator program.
Speaker 1
All right. I'm gonna have a motion to approve. So moved. Moved by Commissioner Kinloch has the support. Support support by Mr. Phillips. Any further discussion? Yes, Miss bola. Yes.
Speaker 19
I'm reporting the number that was in the memo that I have. I'm filling. I'm filling in for a colleague so we'll get the correct number for next week.
Speaker 1
The correct number Well, Mr. Doe, is this a correct number on this board action that we have in front of us?
Speaker 6
To the Chair, Madam Chair, I will go with one the document that is what the board has reviewed if there are any corrections, we will have to bring this back to the board. Okay.
Speaker 1
Thank you seconded as did our CFO. So all right.
Speaker 19
That's fine. I'm sorry, which amount did they sign just so I can know? The 767 Okay. Okay, thank you.
Speaker 1
All  right. Any further discussion? We do have a motion on the floor. All right, hearing none, all in favor signify by saying aye. Aye. Any opposed? Any abstentions? All right. Thank you. Lastly, board action 2423. Yeah, we have a new one. Yeah. Thank you. We have two more. Board action. 2423 West diagnostics. Yes.
right. Any further discussion? We do have a motion on the floor. All right, hearing none, all in favor signify by saying aye. Aye. Any opposed? Any abstentions? All right. Thank you. Lastly, board action 2423. Yeah, we have a new one. Yeah. Thank you. We have two more. Board action. 2423 West diagnostics. Yes.
+1
right. Any further discussion? We do have a motion on the floor. All right, hearing none, all in favor signify by saying aye. Aye. Any opposed? Any abstentions? All right. Thank you. Lastly, board action 2423. Yeah, we have a new one. Yeah. Thank you. We have two more. Board action. 2423 West diagnostics. Yes. Speaker 22
Good  afternoon to this body. Maria Stanfield, director of strategic operations I bring to you board action 2423 request thing $282,988 beginning fiscal year 2024 For October one through 2023. This board action is axing that quest analytics. Be able to provide the software that will assist us with providing network access accuracy, and adequacy analysis based on our population providers and practitioners.
afternoon to this body. Maria Stanfield, director of strategic operations I bring to you board action 2423 request thing $282,988 beginning fiscal year 2024 For October one through 2023. This board action is axing that quest analytics. Be able to provide the software that will assist us with providing network access accuracy, and adequacy analysis based on our population providers and practitioners.
+1
afternoon to this body. Maria Stanfield, director of strategic operations I bring to you board action 2423 request thing $282,988 beginning fiscal year 2024 For October one through 2023. This board action is axing that quest analytics. Be able to provide the software that will assist us with providing network access accuracy, and adequacy analysis based on our population providers and practitioners. Speaker 1
Yeah, motion to approve. So moved by Commissioner Kinloch, supported by Mr. Phillips in the further discussion. See no hands all in favor signify by saying aye. Aye. Any opposed? Any abstentions? All right. Thank you. We do have the one add on that will refer to earlier and that is board action. Tell me the number again. Really 2424 17 Because I didn't write it down. Thank you. All right. All right. Good
Speaker 4
afternoon  again. Cassandra Phipps director. of children's initiatives presenting board action 24 Dash 17 for the school success Health Quality Initiative. This is it will include the School Success Initiative and goal line program. The total funding is $3,530,000. I will note that we do have a new provider there was a request for information process and so team wellness will be the new provider added to the School Success Initiative Program.
again. Cassandra Phipps director. of children's initiatives presenting board action 24 Dash 17 for the school success Health Quality Initiative. This is it will include the School Success Initiative and goal line program. The total funding is $3,530,000. I will note that we do have a new provider there was a request for information process and so team wellness will be the new provider added to the School Success Initiative Program.
+1
again. Cassandra Phipps director. of children's initiatives presenting board action 24 Dash 17 for the school success Health Quality Initiative. This is it will include the School Success Initiative and goal line program. The total funding is $3,530,000. I will note that we do have a new provider there was a request for information process and so team wellness will be the new provider added to the School Success Initiative Program. Speaker 1
All right, is there a motion to approve? Move by Miss Bullock? Is there support support by Mr. Phillips any discussion? Good question. Yes, Mr.
Speaker 7
Schools that the different providers are going to be servicing.
Speaker 4
They should have been added to the board action. But I could double check on that. And if not, I can make sure we can email a copy. Thank you.
Speaker 1
All right, any further discussion or questions? All right, seeing no hands all in favor signify by saying aye. Aye. Any opposed? Any abstentions? one abstention. All right, Commissioner Parker one abstention. All right. Thank you very much. I don't think we have any other board actions. I think that concludes all of our board actions. Trent, is there anyone for good and welfare? Madam Chair? Yes. I just want clarification. Did someone abstain from 2470? Yes, Mr. Pastor Parker. Okay. Thank you so much. Yeah. All right. Okay, Madam Chair. Yes. Yeah, we restate who made the motion, or the motion was made by oh my gosh, we're going so bad yeah, you got it.
Unknown Speaker
This miserable like made the motion to support it. Yeah. Okay. Thank you so much.
Unknown Speaker
Gonna go on pretty quickly. The motion carry. The motion carries. Okay. Okay. All right. Madam Chair.
Unknown Speaker
We do have members of the public with us today.
Speaker 1
So is anybody can you make the announcement about if anybody wants to speak?
Speaker 7
Absolutely. So for those of you who would like to make public comment today, we ask that you do so by using the Raise Your Hand feature.
Speaker 1
Someone raises their hand and I'll read the okay. So far, no hands. Okay. Going once, going twice. Yes. Okay. All right. No public comment, no public comment. It's been requested, and therefore I will not read the good and welfare statement. It's been a very robust meeting. I want to thank all the staff and we've got some good reports. Board members, do you have anything you want to say? Before I call for a motion to adjourn? Any board members have anything they want to say? Goodbye. All right. Goodbye. All right, then. Well, I call for a motion to adjourn. Please. Move by Miss Bullock supported by Mr. Parker. All in favor signify by saying Aye. Any opposed? Any abstentions? All right. We are adjourned. Thank you everybody. Yeah, we are recording stopped