Loading...
Synchron latest developments - Tom Oxley CEO
Speaker 1
thing that was just something that just happened with a the the neuro interventional community has got themselves organized in Britain a little bit more now, I think but so I came to New York to do my neuro interventional fellowship for two years. And in that process, I was trying to translate what had been a research group into a company. And I actually formed a company back in Australia, but it was really just a holding company for for the first patent that I had. So part of the reason I was able to convince the University of Melbourne to let me spin out this company even though I had no experience in doing it and they were really pushing me pushing against me initially, was because I had the patent and I had written the first patent in a year off before I'd started my neurology training read travelled around the world backpacking, but I was like writing patents. And so that was an important lesson like if you're going to write patents, try and do it when you're not employed by some Institute who's going to grab it. All from you. So it meant that I could when I then came back to do my neurology training, I had this patent which I just owned, and like they couldn't spin up the company without me so I forced them to let me run the company. So then I couldn't raise any money in Australia. We're doing well from a grant perspective, I think we raised a total of about the time I left it was about 10 or $15 million in grant funding from us and Australian governments. So very fortunate from that perspective, but to turn it into a company I had to like convince investors that we had a business plan sorry about the long preamble here but just sort of sets the scene. For where we'll go here. So then I came to New York, I do my neuro interventional fellowship, and the guy who was my boss, who's Jay Mako, who's a prolific academic, endovascular neurosurgeon. He's got 600 papers, I think, is also very involved with a lot of companies, startups, and so he was my boss at Mount Sinai. He still was my boss at Mount Sinai in the Department of Neurosurgery. And he introduced me to some investors and I was able to get the first check for the what was the sort of first round of financing and that was a few million dollars to then take our device from what had been a handcrafted animal device to then make a first inhuman device which is pretty ugly, but was enough to convince the Australian FDA that we could enroll some early patients in the first in human study and go from there. So then things kind of rolled on from there, but that's kind of how I got here. So as a neurologist, you know, and now you know, obviously BCI has is a flourishing field and, you know, very famous and rich people now in the space and there's huge amounts of capital flying in which is great for patients. But what I'm going to talk about today is, you know, as a neurologist, as a clinician running the company, I think I've got a real focus on what it's going to take for clinical translation. And I think if I was to say how I'm different from the other BCI CEOs it's they're probably coming at it from a more tech lens and I'm coming at this from you know, my training was in evidence and clinical medicine and understanding what it takes to get into New England Journal of Medicine and what a controlled trial looks like and what the FDA need to see to give approval. So, this talk I'm going to give right now is what what I think is needed for the field to move from the academic scientific preclinical domain of BCI into a fully fledged clinical field clinical medical field. So that's a very long preamble. Sorry about that. Okay. All right.
Speaker 1
So obviously, I'm have disclosures. I'm conflicted with everything I say. So you'll have to take everything I say and ask, you know, ask the question yourself. So this is the system. So there's, there's really there's four components on the left there are that plugs into that. So there's this stent that has sensors on it. That's connected to a lead flexible lead that goes in the blood vessel, and then it plugs into this device which basically brings the raw amplifies filters communicates the data out of the body to this external device that's about the size of an iPhone, it does not have a screen. It receives the it receives the raw brain data. It does the processing, and it can be uploaded from the cloud one day I'd love to merge these two but by bringing this external gives us an ability to upgrade and separate out certain features of the system that helps us with you know, management of algorithms and updates and cloud engagements, you know, because packing everything in here really locks it down from an FDA class three perspective, but it doesn't have a screen and then it creates a server and connects to end devices. This is an iPad with you know, one of our one of our apps on here where the system is being controlled by the user. So the idea is that our patients who have an inability to use their hands to control a smart device or a touchscreen can use this system to then manipulate control the touchscreen so we're up to 10 patients, the 10th patient we had we did four patients in Australia than six patients in a feasibility study in the US and the 10th. Patient was enrolled a couple of weeks ago. So  we're finishing up this feasibility study and the company is at the point where we are building a device ready for commercial grade manufacture, and then presenting that to the FDA and negotiating what we think a pivotal trial should look like. And it's an interesting time for the field because no company I mean, I mean, you know, there's been a lot of work in academically like with BrainGate. And but they've all been academic iterations of, you know, slightly very slight variations on a theme with use cases in an academic setting to prove some level of performance. So what we're now trying to do is get a base level of performance across a range of patients that's usable for a large number of people and proving out that we can demonstrate benefit in a pivotal study which has never been done in BCI. before. And, you know, part of what I'm going to talk about is, it's not obvious how you measure clinical efficacy. With the BCI. There's a face validity to this. There's like, well, you can see the patient doing something and that's beneficial. That's true, but how you quantify things from a clinical perspective
we're finishing up this feasibility study and the company is at the point where we are building a device ready for commercial grade manufacture, and then presenting that to the FDA and negotiating what we think a pivotal trial should look like. And it's an interesting time for the field because no company I mean, I mean, you know, there's been a lot of work in academically like with BrainGate. And but they've all been academic iterations of, you know, slightly very slight variations on a theme with use cases in an academic setting to prove some level of performance. So what we're now trying to do is get a base level of performance across a range of patients that's usable for a large number of people and proving out that we can demonstrate benefit in a pivotal study which has never been done in BCI. before. And, you know, part of what I'm going to talk about is, it's not obvious how you measure clinical efficacy. With the BCI. There's a face validity to this. There's like, well, you can see the patient doing something and that's beneficial. That's true, but how you quantify things from a clinical perspective 
 is is an unanswered question. And I think whatever metric we get to that we're going to present to the FDA and we we have one, which I'm going to describe to you now is going to have an impact on shaping the field to come after us with how we start to do things. And if you look at all of the like nature papers recently coming out, not present a few of them they're all very different. So So I want to talk about four things. One, what is the actual unmet clinical need? Because that is different to the big focus in the BCI world, which is how high can your performance be? How, How good can it how powerful can it be? It's actually a different question to what is the base level of need that the patient has that can we start to address because they don't always match up to what I was just discussing, which is how do you measure clinical meaningful performance? And then I'll explain how we have approached things from the blood vessel and what we think it's going to take to bring this through through clinical translation. Okay, so in recent weeks, you've seen you may have seen these two nature papers come out from the Stanford group, the brain gate group, with Jamie Henderson, and Hochberg and CO as well as the Eddie Chang group and UCSF both phenomenal work and, you know, bringing up to state of the art in BCI. Really high word per minute rates, but still in a pretty, you know, experimental type setting and if, you know, as anyone who studied medicine you would have seen the pictures when you first learn about cardiac pacemakers, and you see what those first cardiac pacemakers looked like leads coming out of the chest, connected to a fridge sighs bit of electronics in the room. I kind of feel like that's what this early BCI is, you know, engineers in the room cables coming out of the skull training periods that go for quite a long time weeks to months. Like that's, it's incredible, but it's not ready for, you know, Primetime clinical translation. And what I find interesting is the first Nature paper came out in 2006. The first human implant was the Scott Ian Kennedy, who there's that Netflix documentary about him you should check out called Father, the cyborg. It's about a Scotsman called Ian Kennedy, who was actually the first neurologists to conduct human clinical trials. Anyway, that's historical but and then Hochberg publication in 2006. What I think is interesting is from 2006 to 2023. We've used the same system in you know, individual use cases where there's been huge improvement, but why is it that there's still no device on market that's available? to patients, these are still only available in a clinical trial setting at a very low number of patients. And we're still using a very similar system and it just, it speaks to how hard it is to to achieve clinical translation in this field. Now neuro link have come along and your link have already spent around $300 million, and they're still not in a human clinical trial testing and they're going to get there. But you know, does it take $300 million? No, we we think we're getting close but we made a bunch of design decisions to really simplify down the system to make it easy to use but also manufacturable scalable, and repeatable. So, you know, so I want to just speak around
is is an unanswered question. And I think whatever metric we get to that we're going to present to the FDA and we we have one, which I'm going to describe to you now is going to have an impact on shaping the field to come after us with how we start to do things. And if you look at all of the like nature papers recently coming out, not present a few of them they're all very different. So So I want to talk about four things. One, what is the actual unmet clinical need? Because that is different to the big focus in the BCI world, which is how high can your performance be? How, How good can it how powerful can it be? It's actually a different question to what is the base level of need that the patient has that can we start to address because they don't always match up to what I was just discussing, which is how do you measure clinical meaningful performance? And then I'll explain how we have approached things from the blood vessel and what we think it's going to take to bring this through through clinical translation. Okay, so in recent weeks, you've seen you may have seen these two nature papers come out from the Stanford group, the brain gate group, with Jamie Henderson, and Hochberg and CO as well as the Eddie Chang group and UCSF both phenomenal work and, you know, bringing up to state of the art in BCI. Really high word per minute rates, but still in a pretty, you know, experimental type setting and if, you know, as anyone who studied medicine you would have seen the pictures when you first learn about cardiac pacemakers, and you see what those first cardiac pacemakers looked like leads coming out of the chest, connected to a fridge sighs bit of electronics in the room. I kind of feel like that's what this early BCI is, you know, engineers in the room cables coming out of the skull training periods that go for quite a long time weeks to months. Like that's, it's incredible, but it's not ready for, you know, Primetime clinical translation. And what I find interesting is the first Nature paper came out in 2006. The first human implant was the Scott Ian Kennedy, who there's that Netflix documentary about him you should check out called Father, the cyborg. It's about a Scotsman called Ian Kennedy, who was actually the first neurologists to conduct human clinical trials. Anyway, that's historical but and then Hochberg publication in 2006. What I think is interesting is from 2006 to 2023. We've used the same system in you know, individual use cases where there's been huge improvement, but why is it that there's still no device on market that's available? to patients, these are still only available in a clinical trial setting at a very low number of patients. And we're still using a very similar system and it just, it speaks to how hard it is to to achieve clinical translation in this field. Now neuro link have come along and your link have already spent around $300 million, and they're still not in a human clinical trial testing and they're going to get there. But you know, does it take $300 million? No, we we think we're getting close but we made a bunch of design decisions to really simplify down the system to make it easy to use but also manufacturable scalable, and repeatable. So, you know, so I want to just speak around  there was a really nice Nathan crone is a neurologist in the US. He's at Johns Hopkins, who's done a lot of BCI work, and Nick Ramsey is in the Netherlands in Utrecht. He's a neuroscientist who published a paper I'll show you in a minute, but the two of them got together to write a opinion piece on how we should think about these latest latest technologies. And I I'm, you know, the way they've said this was I just want to talk about this because it's really well put. So number one, you have to make it fully implantable. They said high bandwidth recordings were taken from hundreds of electrodes which had to be connected to external amplifiers through a pedestal penetrates the skin which is cosmetic typically unappealing. I think that's you know, euphemistic to say, cosmetically unappealing I you know, patients that don't like it, but the biggest risk is that you constantly have an infection risk. That's the more concerning thing with this. So, there's a reason you know, the Pacemakers became fully implantable. Troubleshooting highly skilled researchers were actively involved in the operation of reported BCIs, which remained too complicated for caregivers to operate in home settings without extensive training and maintenance. So I characterize that as troubleshooting. It's just not something that you might think about. But if you have a bunch of engineers having to make this work in the room, which is the case with every single BCI demonstration, that's been reported in the literature, you have to solve for that. And that is there's so many things to troubleshoot, and part of it is the complexity of the needs of the system to start being effective. So you have to remove all of those needs. If you're going to build something at scale. It just has to work and not have to be troubleshot. Because you're you're talking about patients that are severely impaired, they can't do any troubleshooting. And if there's a need to fix things along the way, you've defeated the whole purpose of what you're trying to do. And then stability. So I think mea stands for I can't remember the is it multi unit, I can't remember, they're talking about penetrating arrays. Signals tend to be unstable and require frequent updating of speech decoding models might be limited by degradation of electrode materials, and tissue encapsulation of the devices. So they're different things electrode of the materials is is a question because there has been an increasing introduction of polymers into implants where there's a you know, I was just saying to Andreas and will, there is a question mark over the longevity and degradation of polymers if you put a polymer into the brain. Now, we're seeing that with epilepsy applications, but if you go for devices that need to withstand, you know, a lifetime, and you put them on a polymer polymers degrade. So that's a big question. Tissue encapsulation is different tissue encapsulation is that the if you're going to penetrate into brain parenchyma
there was a really nice Nathan crone is a neurologist in the US. He's at Johns Hopkins, who's done a lot of BCI work, and Nick Ramsey is in the Netherlands in Utrecht. He's a neuroscientist who published a paper I'll show you in a minute, but the two of them got together to write a opinion piece on how we should think about these latest latest technologies. And I I'm, you know, the way they've said this was I just want to talk about this because it's really well put. So number one, you have to make it fully implantable. They said high bandwidth recordings were taken from hundreds of electrodes which had to be connected to external amplifiers through a pedestal penetrates the skin which is cosmetic typically unappealing. I think that's you know, euphemistic to say, cosmetically unappealing I you know, patients that don't like it, but the biggest risk is that you constantly have an infection risk. That's the more concerning thing with this. So, there's a reason you know, the Pacemakers became fully implantable. Troubleshooting highly skilled researchers were actively involved in the operation of reported BCIs, which remained too complicated for caregivers to operate in home settings without extensive training and maintenance. So I characterize that as troubleshooting. It's just not something that you might think about. But if you have a bunch of engineers having to make this work in the room, which is the case with every single BCI demonstration, that's been reported in the literature, you have to solve for that. And that is there's so many things to troubleshoot, and part of it is the complexity of the needs of the system to start being effective. So you have to remove all of those needs. If you're going to build something at scale. It just has to work and not have to be troubleshot. Because you're you're talking about patients that are severely impaired, they can't do any troubleshooting. And if there's a need to fix things along the way, you've defeated the whole purpose of what you're trying to do. And then stability. So I think mea stands for I can't remember the is it multi unit, I can't remember, they're talking about penetrating arrays. Signals tend to be unstable and require frequent updating of speech decoding models might be limited by degradation of electrode materials, and tissue encapsulation of the devices. So they're different things electrode of the materials is is a question because there has been an increasing introduction of polymers into implants where there's a you know, I was just saying to Andreas and will, there is a question mark over the longevity and degradation of polymers if you put a polymer into the brain. Now, we're seeing that with epilepsy applications, but if you go for devices that need to withstand, you know, a lifetime, and you put them on a polymer polymers degrade. So that's a big question. Tissue encapsulation is different tissue encapsulation is that the if you're going to penetrate into brain parenchyma
+1
we're finishing up this feasibility study and the company is at the point where we are building a device ready for commercial grade manufacture, and then presenting that to the FDA and negotiating what we think a pivotal trial should look like. And it's an interesting time for the field because no company I mean, I mean, you know, there's been a lot of work in academically like with BrainGate. And but they've all been academic iterations of, you know, slightly very slight variations on a theme with use cases in an academic setting to prove some level of performance. So what we're now trying to do is get a base level of performance across a range of patients that's usable for a large number of people and proving out that we can demonstrate benefit in a pivotal study which has never been done in BCI. before. And, you know, part of what I'm going to talk about is, it's not obvious how you measure clinical efficacy. With the BCI. There's a face validity to this. There's like, well, you can see the patient doing something and that's beneficial. That's true, but how you quantify things from a clinical perspective +2
is is an unanswered question. And I think whatever metric we get to that we're going to present to the FDA and we we have one, which I'm going to describe to you now is going to have an impact on shaping the field to come after us with how we start to do things. And if you look at all of the like nature papers recently coming out, not present a few of them they're all very different. So So I want to talk about four things. One, what is the actual unmet clinical need? Because that is different to the big focus in the BCI world, which is how high can your performance be? How, How good can it how powerful can it be? It's actually a different question to what is the base level of need that the patient has that can we start to address because they don't always match up to what I was just discussing, which is how do you measure clinical meaningful performance? And then I'll explain how we have approached things from the blood vessel and what we think it's going to take to bring this through through clinical translation. Okay, so in recent weeks, you've seen you may have seen these two nature papers come out from the Stanford group, the brain gate group, with Jamie Henderson, and Hochberg and CO as well as the Eddie Chang group and UCSF both phenomenal work and, you know, bringing up to state of the art in BCI. Really high word per minute rates, but still in a pretty, you know, experimental type setting and if, you know, as anyone who studied medicine you would have seen the pictures when you first learn about cardiac pacemakers, and you see what those first cardiac pacemakers looked like leads coming out of the chest, connected to a fridge sighs bit of electronics in the room. I kind of feel like that's what this early BCI is, you know, engineers in the room cables coming out of the skull training periods that go for quite a long time weeks to months. Like that's, it's incredible, but it's not ready for, you know, Primetime clinical translation. And what I find interesting is the first Nature paper came out in 2006. The first human implant was the Scott Ian Kennedy, who there's that Netflix documentary about him you should check out called Father, the cyborg. It's about a Scotsman called Ian Kennedy, who was actually the first neurologists to conduct human clinical trials. Anyway, that's historical but and then Hochberg publication in 2006. What I think is interesting is from 2006 to 2023. We've used the same system in you know, individual use cases where there's been huge improvement, but why is it that there's still no device on market that's available? to patients, these are still only available in a clinical trial setting at a very low number of patients. And we're still using a very similar system and it just, it speaks to how hard it is to to achieve clinical translation in this field. Now neuro link have come along and your link have already spent around $300 million, and they're still not in a human clinical trial testing and they're going to get there. But you know, does it take $300 million? No, we we think we're getting close but we made a bunch of design decisions to really simplify down the system to make it easy to use but also manufacturable scalable, and repeatable. So, you know, so I want to just speak around +1
there was a really nice Nathan crone is a neurologist in the US. He's at Johns Hopkins, who's done a lot of BCI work, and Nick Ramsey is in the Netherlands in Utrecht. He's a neuroscientist who published a paper I'll show you in a minute, but the two of them got together to write a opinion piece on how we should think about these latest latest technologies. And I I'm, you know, the way they've said this was I just want to talk about this because it's really well put. So number one, you have to make it fully implantable. They said high bandwidth recordings were taken from hundreds of electrodes which had to be connected to external amplifiers through a pedestal penetrates the skin which is cosmetic typically unappealing. I think that's you know, euphemistic to say, cosmetically unappealing I you know, patients that don't like it, but the biggest risk is that you constantly have an infection risk. That's the more concerning thing with this. So, there's a reason you know, the Pacemakers became fully implantable. Troubleshooting highly skilled researchers were actively involved in the operation of reported BCIs, which remained too complicated for caregivers to operate in home settings without extensive training and maintenance. So I characterize that as troubleshooting. It's just not something that you might think about. But if you have a bunch of engineers having to make this work in the room, which is the case with every single BCI demonstration, that's been reported in the literature, you have to solve for that. And that is there's so many things to troubleshoot, and part of it is the complexity of the needs of the system to start being effective. So you have to remove all of those needs. If you're going to build something at scale. It just has to work and not have to be troubleshot. Because you're you're talking about patients that are severely impaired, they can't do any troubleshooting. And if there's a need to fix things along the way, you've defeated the whole purpose of what you're trying to do. And then stability. So I think mea stands for I can't remember the is it multi unit, I can't remember, they're talking about penetrating arrays. Signals tend to be unstable and require frequent updating of speech decoding models might be limited by degradation of electrode materials, and tissue encapsulation of the devices. So they're different things electrode of the materials is is a question because there has been an increasing introduction of polymers into implants where there's a you know, I was just saying to Andreas and will, there is a question mark over the longevity and degradation of polymers if you put a polymer into the brain. Now, we're seeing that with epilepsy applications, but if you go for devices that need to withstand, you know, a lifetime, and you put them on a polymer polymers degrade. So that's a big question. Tissue encapsulation is different tissue encapsulation is that the if you're going to penetrate into brain parenchyma Speaker 1
then you have to deal with gliosis and gliosis is unlike scarring on the skin where you get a scar tissue and then it stops. You have college inflammation, and then the process stops. gliosis does not to stop if there is a foreign body. It's just the nature of you know, being on that side of the blood brain barrier and the way that healing happens in the brain. And so as the as the glottic scars form and continue to form there is a change in the impedance measurements because the impedance measurements are so sensitive at the multi unit or single unit recording level, that the change in impedance that happens over time with glottic reactions can impact signal stability. And so what the way that if that's not actually a safety concern, because it's not going to hurt the patient, but it's an efficacy concern, because you might then need to continually recalibrate the system because you have an ongoing dynamic biological interface issue. So one way to avoid that is to try to avoid penetration into the brain whatsoever. So the ECOG electrodes potentially do that they sit on the surface of the brain, but they still do elicit some sufficient tissue reactions, but probably less than the penetrating, but obviously you give up so you know, you know, I'm noticing I think a discussion happening at the, at the, at the conferences, amongst the key opinion leaders that it seems to be the thought that ECOG is a nice kind of middle ground. But there's a question there are still lots of questions over Can you remove the ECOG How do you patio What about the polymer back descargue? What are the tissue reactions? So but that's what Eddie Chang's group is using? ACOG electrodes. Okay. So so that just kind of sets the scene for why there's been an issue on the technology side now I just want to talk a little bit about what does all that mean for patients and we've been doing a lot of thinking about and talking to patients about what their needs are. And I guess just to reiterate, reiterate the point. It's not useful if you build a high performance system for a patient that needs to have troubleshooting at a regular interval because it will stop working. So we've come up with this term, continuous digital autonomy and the way I'd think about that is that feeling you get when maybe your phone dies or you wake up in the morning and you can't quite reach your phone or it's or you've lost it, that moment where you go, Oh, shit, where's my phone? And you've lost that connection to your digital world. Think about that. But your arms don't work anymore. So you have an injury, you have some sort of disease, you lose your access to the digital ecosystem, which is extremely powerful. You want that back and you want it back all the time. So this idea and so autonomy is this idea that you can have agency in the world independently. Autonomy is your ability to, you know, you know, have sovereignty in your own self not have to depend on anyone else. So, continuous digital autonomy. That's, I think, what BCI is a problem that BCI can potentially solve. So Nick Ramsey in his New England Journal paper, which I'll get to in a sec wrote for BCI to provide meaningful benefit in the real world. It must allow for user autonomy and continuous functionality. So, you know, we have taken that very seriously now. And you know, Ramsey was at the BCI conference in Brussels this year in June. And at one point he said to the world, he here sort of announced at the conference, you know, he sort of stood up and he said, these five things you said, it's got to be easily easy to learn how to use low cognitive effort for the patient. It's got to be easy to use with low recalibration, ideally less than every two weeks. It should work immediately. You shouldn't have to train for days, weeks or even months to make it work. It should work 24/7 And it should be stable. So I thought I've captured that as what I'm calling the Ramsey five as a kind of design ethos for how we're trying to build a system. So, you know, we have a low channel count system, and the only New England so New England Journal of Medicine is the gold standard. Well, this kind of three journals of gold standard clinical medicine, right. There's New England Journal, there's Lancet, and there's probably Jama I think New England Journal has the highest highest impact factor. And it is the kind of gold standard for clinical medicine. So to get into New England Journal of Medicine, you really have to have achieved some serious level of clinical meaningfulness. So Nick Ramsey and his group put in a low channel count system into the brain they made it fully implantable and it only delivered a single click System, but the patient was able to then engage with the software where she previously needed someone, a nurse or someone next to a printer, trying to guess what she wanted to select. Or she could use eye gaze but she had issues  with eye gaze couldn't use eye gaze outside. And eye gaze has its own issues with constant recalibration. And so this system has become her she has been using this now for seven years. And the eye tracking has you know, been there at times but it's not always her full back and this now has become a fullback and she can, as you see, go outside with the system. So I think this was you know, it's not really talked about this paper very much because it doesn't have the flashy 50 words per minute rating, which is what the whole world is fixated on is words per minute, or like how powerful the system can be. This is the only BCI paper that's in New England Journal of Medicine and it's because it's actually focused on what the patient need is. So for me, this is my most inspiring paper and what we're trying to build towards Tim Dennison. I don't know if he's on the call, but Tim Dennison was on this paper as well. This was actually the Medtronic system that Tim, his team built at Medtronic when he was there. And so Tim was a
with eye gaze couldn't use eye gaze outside. And eye gaze has its own issues with constant recalibration. And so this system has become her she has been using this now for seven years. And the eye tracking has you know, been there at times but it's not always her full back and this now has become a fullback and she can, as you see, go outside with the system. So I think this was you know, it's not really talked about this paper very much because it doesn't have the flashy 50 words per minute rating, which is what the whole world is fixated on is words per minute, or like how powerful the system can be. This is the only BCI paper that's in New England Journal of Medicine and it's because it's actually focused on what the patient need is. So for me, this is my most inspiring paper and what we're trying to build towards Tim Dennison. I don't know if he's on the call, but Tim Dennison was on this paper as well. This was actually the Medtronic system that Tim, his team built at Medtronic when he was there. And so Tim was a  very early inspiration for my team and worked closely with my team as we're thinking about this sort of solution case as a design inspiration. Okay, there's more to come on this by the way, like we are still working on the patient need one of my close collaborators and other Australian who's here in New York called David Petrino, who is a physical therapist, physiotherapist, PhD, who works with patients a lot. He's doing a lot of the work on thinking about the patient need and starting to build a scale that we think is going to be useful. But you know, this is an area that is kind of I think neglected but it's really important for BCI to make it into the clinical domain so that physicians can start discussing what matters and what doesn't matter. Okay, I've kind of talked about this a little bit, but I'm now going to make an argument for how I think how we came to a clinical metric, which is not what you would typically see with BCI and so part of that is the burden is on us to describe how a motor BCI restores a bodily function. And so that, you know, you guys have used the term neuroprosthesis I think the term neuroprosthesis is really interesting. I think it's not necessarily synonymous with brain computer interface. neuroprosthesis means that you have a medical device that restores a brain function. brain computer interface means that you have a device that connects the brain to an outside device, an external device and perform some function. The difference there is that neuroprosthesis infers some restoration of a bodily function, which is not inferred in BCI. And that's really important for I think, from a clinical science perspective, because it's good to point towards how you're what function you're restoring. So the way I'm thinking about this is the FDA used the term motor capability. So you know, as a neurologist, we don't really talk about the motor system in you know, this simplistic term, but I think it's been a really important way to think about it. Motor intent, which again, I don't really talk about much as a neurologist because it's just the function of the motor cortex. So if you have a cortical stroke, you have motor impairment, like you have, you know, a spastic paraparesis Am I speaking like an American now Hemi presses, power presses I'm seeing like an American but motor intent is captured through function in the cortex, motor transmission is is conducted by the the motor neurons, secondary second order and that tertiary auto motor neurons which run from the cortex, brainstem, spinal cord, peripheral nerves, and then eventually they innovate a motor, a motor complex, which then activates control over the joint and you eventually then click on Google Maps on your screen on your iPhone. So, you know, I'm kind of incorporating the iPhone almost into the motor system because what we're talking about is a bypass. Well firstly, just talk about the conditions that can cause this but you know, we're looking at the end use not necessarily of restoration of the joints and muscles, but the restoration of a digital system. So we're thinking about the problem and how does the motor system control a smartphone because we know that this can deliver so much of what your life needs, which I'll get to in a sec.
very early inspiration for my team and worked closely with my team as we're thinking about this sort of solution case as a design inspiration. Okay, there's more to come on this by the way, like we are still working on the patient need one of my close collaborators and other Australian who's here in New York called David Petrino, who is a physical therapist, physiotherapist, PhD, who works with patients a lot. He's doing a lot of the work on thinking about the patient need and starting to build a scale that we think is going to be useful. But you know, this is an area that is kind of I think neglected but it's really important for BCI to make it into the clinical domain so that physicians can start discussing what matters and what doesn't matter. Okay, I've kind of talked about this a little bit, but I'm now going to make an argument for how I think how we came to a clinical metric, which is not what you would typically see with BCI and so part of that is the burden is on us to describe how a motor BCI restores a bodily function. And so that, you know, you guys have used the term neuroprosthesis I think the term neuroprosthesis is really interesting. I think it's not necessarily synonymous with brain computer interface. neuroprosthesis means that you have a medical device that restores a brain function. brain computer interface means that you have a device that connects the brain to an outside device, an external device and perform some function. The difference there is that neuroprosthesis infers some restoration of a bodily function, which is not inferred in BCI. And that's really important for I think, from a clinical science perspective, because it's good to point towards how you're what function you're restoring. So the way I'm thinking about this is the FDA used the term motor capability. So you know, as a neurologist, we don't really talk about the motor system in you know, this simplistic term, but I think it's been a really important way to think about it. Motor intent, which again, I don't really talk about much as a neurologist because it's just the function of the motor cortex. So if you have a cortical stroke, you have motor impairment, like you have, you know, a spastic paraparesis Am I speaking like an American now Hemi presses, power presses I'm seeing like an American but motor intent is captured through function in the cortex, motor transmission is is conducted by the the motor neurons, secondary second order and that tertiary auto motor neurons which run from the cortex, brainstem, spinal cord, peripheral nerves, and then eventually they innovate a motor, a motor complex, which then activates control over the joint and you eventually then click on Google Maps on your screen on your iPhone. So, you know, I'm kind of incorporating the iPhone almost into the motor system because what we're talking about is a bypass. Well firstly, just talk about the conditions that can cause this but you know, we're looking at the end use not necessarily of restoration of the joints and muscles, but the restoration of a digital system. So we're thinking about the problem and how does the motor system control a smartphone because we know that this can deliver so much of what your life needs, which I'll get to in a sec.
+1
with eye gaze couldn't use eye gaze outside. And eye gaze has its own issues with constant recalibration. And so this system has become her she has been using this now for seven years. And the eye tracking has you know, been there at times but it's not always her full back and this now has become a fullback and she can, as you see, go outside with the system. So I think this was you know, it's not really talked about this paper very much because it doesn't have the flashy 50 words per minute rating, which is what the whole world is fixated on is words per minute, or like how powerful the system can be. This is the only BCI paper that's in New England Journal of Medicine and it's because it's actually focused on what the patient need is. So for me, this is my most inspiring paper and what we're trying to build towards Tim Dennison. I don't know if he's on the call, but Tim Dennison was on this paper as well. This was actually the Medtronic system that Tim, his team built at Medtronic when he was there. And so Tim was a +1
very early inspiration for my team and worked closely with my team as we're thinking about this sort of solution case as a design inspiration. Okay, there's more to come on this by the way, like we are still working on the patient need one of my close collaborators and other Australian who's here in New York called David Petrino, who is a physical therapist, physiotherapist, PhD, who works with patients a lot. He's doing a lot of the work on thinking about the patient need and starting to build a scale that we think is going to be useful. But you know, this is an area that is kind of I think neglected but it's really important for BCI to make it into the clinical domain so that physicians can start discussing what matters and what doesn't matter. Okay, I've kind of talked about this a little bit, but I'm now going to make an argument for how I think how we came to a clinical metric, which is not what you would typically see with BCI and so part of that is the burden is on us to describe how a motor BCI restores a bodily function. And so that, you know, you guys have used the term neuroprosthesis I think the term neuroprosthesis is really interesting. I think it's not necessarily synonymous with brain computer interface. neuroprosthesis means that you have a medical device that restores a brain function. brain computer interface means that you have a device that connects the brain to an outside device, an external device and perform some function. The difference there is that neuroprosthesis infers some restoration of a bodily function, which is not inferred in BCI. And that's really important for I think, from a clinical science perspective, because it's good to point towards how you're what function you're restoring. So the way I'm thinking about this is the FDA used the term motor capability. So you know, as a neurologist, we don't really talk about the motor system in you know, this simplistic term, but I think it's been a really important way to think about it. Motor intent, which again, I don't really talk about much as a neurologist because it's just the function of the motor cortex. So if you have a cortical stroke, you have motor impairment, like you have, you know, a spastic paraparesis Am I speaking like an American now Hemi presses, power presses I'm seeing like an American but motor intent is captured through function in the cortex, motor transmission is is conducted by the the motor neurons, secondary second order and that tertiary auto motor neurons which run from the cortex, brainstem, spinal cord, peripheral nerves, and then eventually they innovate a motor, a motor complex, which then activates control over the joint and you eventually then click on Google Maps on your screen on your iPhone. So, you know, I'm kind of incorporating the iPhone almost into the motor system because what we're talking about is a bypass. Well firstly, just talk about the conditions that can cause this but you know, we're looking at the end use not necessarily of restoration of the joints and muscles, but the restoration of a digital system. So we're thinking about the problem and how does the motor system control a smartphone because we know that this can deliver so much of what your life needs, which I'll get to in a sec. Speaker 1
So if you think about it from that perspective, a motor BCI can help a lot of people you know, maybe not cortical stroke because you need the cortex to generate your motor intent. subcortical stroke or maybe Perry cortical stroke, spinal cord injury, peripheral nerve disease, GBS CIDP, muscle disease, muscular dystrophy, multifocal motor neuropathy arthroplasties and then neurodegenerative conditions like ALS but then there's other sort of, you know, that's paralysis, but if you think about motor impairment, then you've got cerebral palsy, Parkinson's disease, the kind of, you know, dystonia is the kind of positive phenomenon, motor system diseases, but really, you know, anyone who can't make the selection on an iPhone there that can't use their fingers to hit a selection on the screen, that's who we think we can help. And so that, you know, there's been a thought or belief that BCI can only help a tiny group of patients but not really and so, from that perspective, you've got a neuroprosthesis that can solve a broad problem in the same way that the cochlea hearing implant which came out of the same University of Melbourne that we came out of as well. Cochlear back in the 70s came out at University of Melbourne. That was the first and is the only real archetypal neuroprosthesis device on market. Now that stimulation but it's a brain implant or head implant that restores a brain function. And now, you know, this new wave of BCI is a really moto BCIs I know neural link I'm talking about vision a little bit so and then you know, maxtow next group of scientists talking about vision so there's the vision stuff has been had a couple of false starts, but this wave that I think we're seeing right now is really in the domain of motor, and then there's speech and you know, you can Eddie Chang's group, for the most part is decoding motor control of speech, but you could start to argue that speech neuroprosthetics can move away from just motor representations of speech into content of speech and associations of speech. So that's raises an interesting question. So I kind of also probably dropped speech into a different space, but I for me, motor decoding is much more potentially powerful than speech because speech is quite a specific thing. It's like trying to decode a word but a motor prosthesis is kind of like replacing a mouse or a keyboard. It's got widespread applicable use. Yeah, so So with that concept, the motor neuroprosthesis are what we're calling MNP restores the transmission of motor intent. So now we've got a kind of very focal, clinical driven thing that if we can prove, can we prove that we've restored the transmission of motor intent we boil that down to a unit of clinical meaningfulness. And so we came up with this idea of the Petrino has really Petrino just wrote a paper on this digital motor output. And that idea is that we convert a unit of cortical activity of representation of motor intent into a output DMO digital motor output that is able to make a selection on a screen. And if so, if we can just capture that concept of a demo, then we have a base unit of efficacy that we can start to dissect and give to clinicians as a unit of measure of efficacy. of the system. And it kind of becomes interesting from a clinical perspective because, you know, like when you're assessing, you know, when patients come into the emergency room sometimes and they look like they're having a stroke, but they've actually had a stroke in the past and they've now got a urinary tract infection or sepsis and that can make your motor system, you know, deteriorate for it. And so sometimes you think they're having a stroke, but actually they're just got sepsis. So systemic issues can impact the brain's ability to express itself in the motor system. It's going to be the same with the BCI. The clinician is going to have patients coming in with the BCI. And the BCI has stopped working. Why so they're going to have to start assessing the system the same way that they would assess why the limbs or the muscles in the body have stopped working. And so what they'd go and do is look at the numbers or the like analytics behind the digital motor output and it gives you this readout into what's happening at the brain level. And so you can see why that becomes so important probably for the neurologist who is going to be the one called in the ER to come and assess the patient who's presenting with a failed use of as BCI. Will How long am I talking for I'm kind of just crapping on a little bit here.
Speaker 2
That we said sort of 50 minutes of talking 10 minutes for questions. All right.
Speaker 1
So keep going. We've got about No I'll do another 10 or so minutes. Yeah, and then so you know, so this becomes a core unit and then it's a matter of it's not enough on its own is it you have to use this to do something meaningful. And so, you know, we will achieve clinical translation when we can convince Medicare or in the US it's got to be private health insurance in the UK, it's harder BArkas you've got to convince NHS but in the US you've got to convince Medicare and or private insurers to pay for the system for their patients. So that becomes your kind of use case. And so if I take the DMO argument, and I go to a health insurance agency in the US and I say are your patients going to use this to watch Netflix, they're gonna say, we're not paying for that. But if you tell them that you're going to use it to restore their ability to engage in a communication dialogue with their physician over an app or pay their finances or you know, reduce the number of hours of their caregiver because they can do their 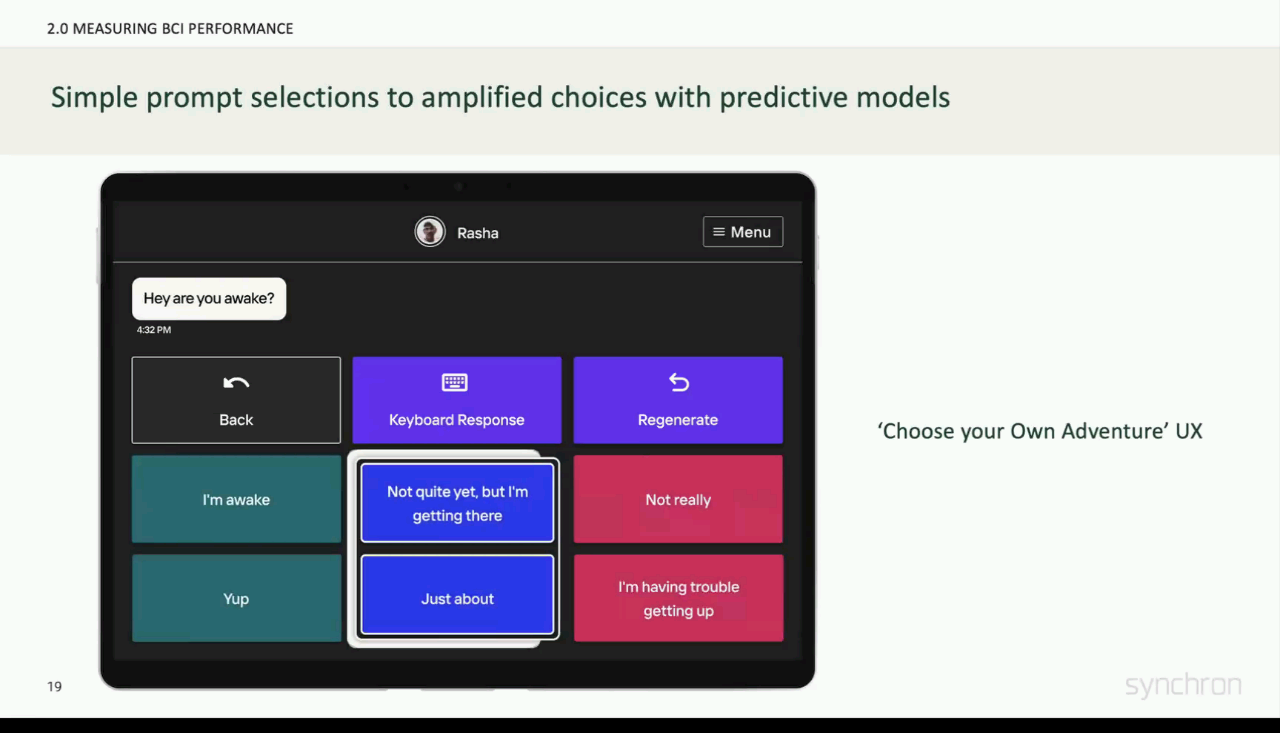
 own shopping or because they can, you know, communicate with communicate their symptoms. You're starting to see how the use of the DMO in a meaningful in a health economics meaningful way. Really Matters for clinical trials success. Okay. You Yeah, I might just keep going here. But you know, I do recommend this Petrino paper that came out in Journal of neuro dimensional surgery this year is he's done a really good job of mapping out how to think about a digital motor output. Go and have, check out that paper so I think we spoke about that. So, you know, I think just to make the point we've missed you know, with a low output system so if you know where we'd like to get to is complete point and click like a mouse moving a cursor around the screen and then a click. We have not gotten to that yet. We've got to a low number of clicks. But not we haven't, we haven't solved two dimensional control. So So we've calling our system a synchronous switch because it's kind of built around these discrete key press outputs. But because it's simple and stable and easy to
own shopping or because they can, you know, communicate with communicate their symptoms. You're starting to see how the use of the DMO in a meaningful in a health economics meaningful way. Really Matters for clinical trials success. Okay. You Yeah, I might just keep going here. But you know, I do recommend this Petrino paper that came out in Journal of neuro dimensional surgery this year is he's done a really good job of mapping out how to think about a digital motor output. Go and have, check out that paper so I think we spoke about that. So, you know, I think just to make the point we've missed you know, with a low output system so if you know where we'd like to get to is complete point and click like a mouse moving a cursor around the screen and then a click. We have not gotten to that yet. We've got to a low number of clicks. But not we haven't, we haven't solved two dimensional control. So So we've calling our system a synchronous switch because it's kind of built around these discrete key press outputs. But because it's simple and stable and easy to 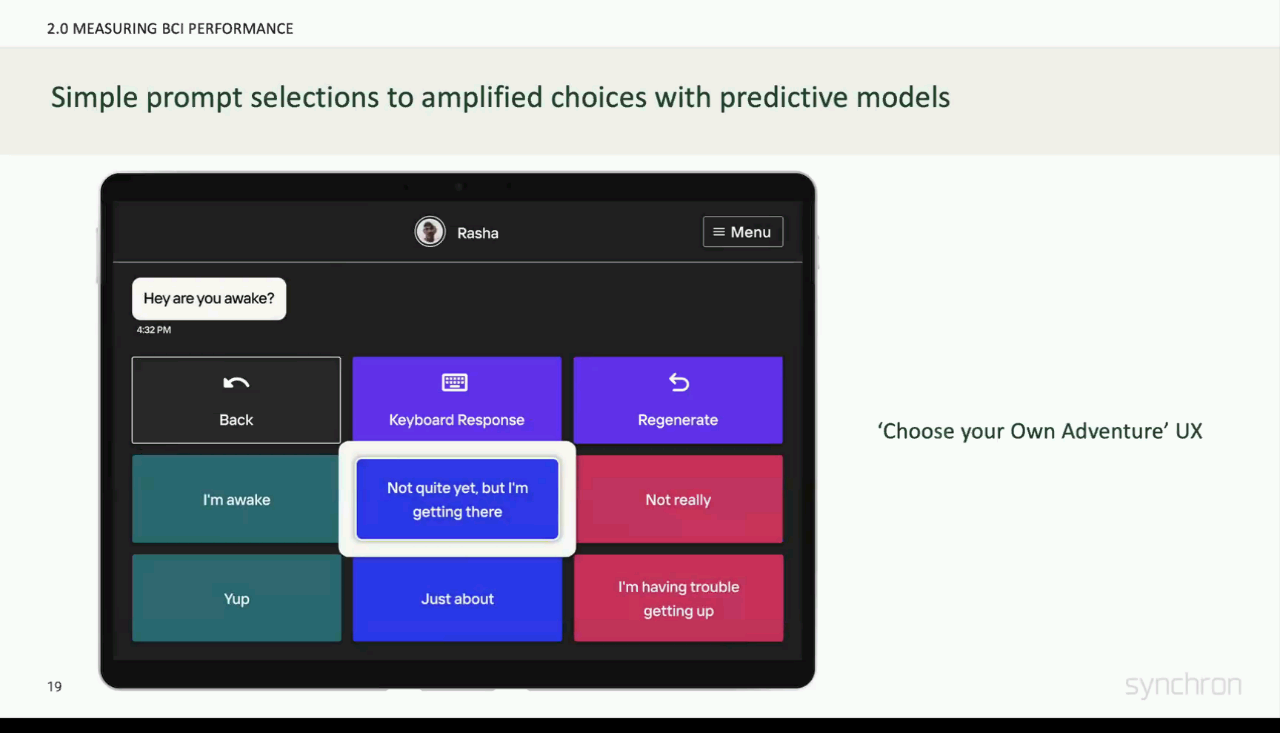
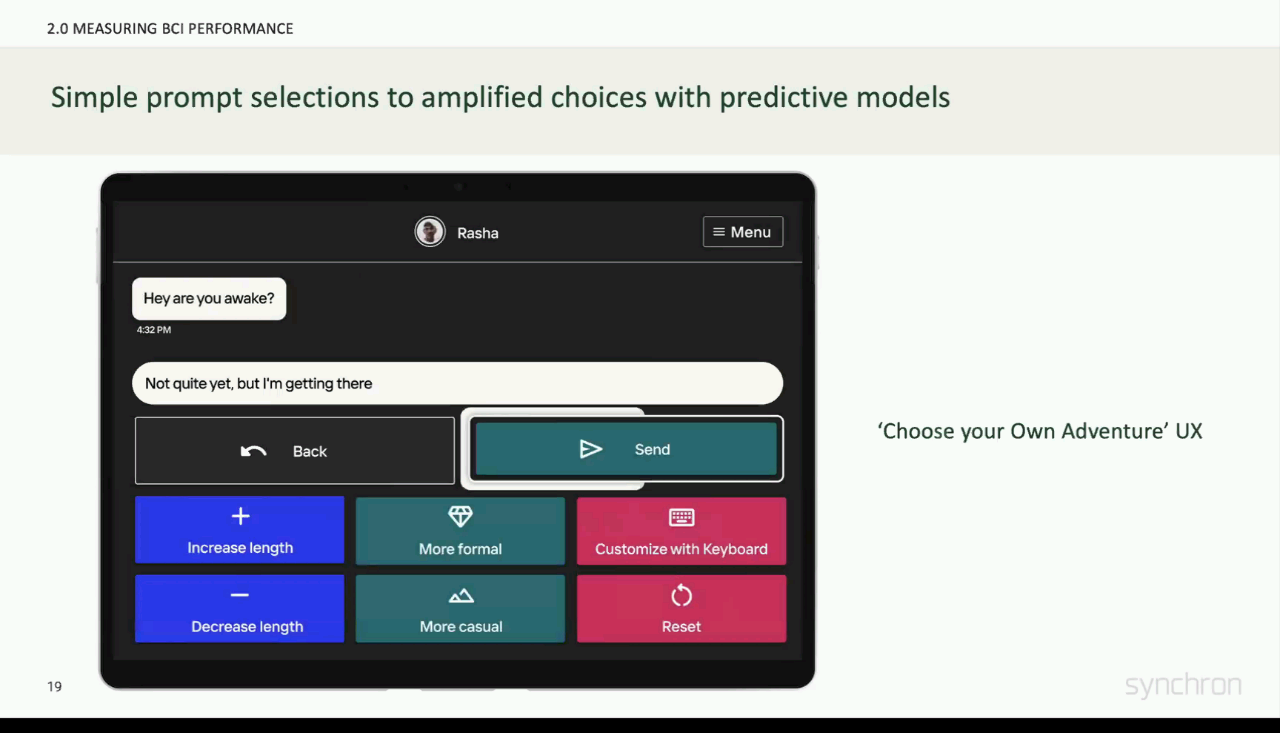 use and work straight away for the patience, we're now building these layers on top and this is just an example where as distinct from, you know, moving the cursor around the screen to make selections of letters, using something like chat GPT or an LLM to start building out predictions of like sentences and phrases. That's context dependent. Our patients love this because they're able to have much more rich conversations and they what they were having before and it's just been a really simple merging of our kind of simple, dependable output with a really high you know, output model that uses LLM. So I think the LLM are going to be this is how LLM 's are going to impact our life. The LLM 's are impacting everyone's what everyone's doing in the world. For us. It's hugely meaningful because it is this great leveler where it gives access to our patients. To really complicated outputs. Okay, so here's one of our patients in he's in New York. This gentleman was told he would have not been with us 10 years ago. He's got ALS. He's had ALS for I think 15 years and he was totally dependent on other people all the time. He can only he can move his eyes a little bit and you can set your same smile at the end of this. This was the first session he turned on he started using the iPhone with his low number low click System. Why this is so meaningful for him is because he has this man has zero privacy. If he ever needs anything someone has to come in and try and interpret what he's looking for. So I'll hit play here. But what you're going to see is him sending these key
use and work straight away for the patience, we're now building these layers on top and this is just an example where as distinct from, you know, moving the cursor around the screen to make selections of letters, using something like chat GPT or an LLM to start building out predictions of like sentences and phrases. That's context dependent. Our patients love this because they're able to have much more rich conversations and they what they were having before and it's just been a really simple merging of our kind of simple, dependable output with a really high you know, output model that uses LLM. So I think the LLM are going to be this is how LLM 's are going to impact our life. The LLM 's are impacting everyone's what everyone's doing in the world. For us. It's hugely meaningful because it is this great leveler where it gives access to our patients. To really complicated outputs. Okay, so here's one of our patients in he's in New York. This gentleman was told he would have not been with us 10 years ago. He's got ALS. He's had ALS for I think 15 years and he was totally dependent on other people all the time. He can only he can move his eyes a little bit and you can set your same smile at the end of this. This was the first session he turned on he started using the iPhone with his low number low click System. Why this is so meaningful for him is because he has this man has zero privacy. If he ever needs anything someone has to come in and try and interpret what he's looking for. So I'll hit play here. But what you're going to see is him sending these key  presses to make selections on this app which is going to report pain for him. So this is one of the applications of the system where users are able to navigate their way through, particularly an iPhone you use it on their own
presses to make selections on this app which is going to report pain for him. So this is one of the applications of the system where users are able to navigate their way through, particularly an iPhone you use it on their own
+2
own shopping or because they can, you know, communicate with communicate their symptoms. You're starting to see how the use of the DMO in a meaningful in a health economics meaningful way. Really Matters for clinical trials success. Okay. You Yeah, I might just keep going here. But you know, I do recommend this Petrino paper that came out in Journal of neuro dimensional surgery this year is he's done a really good job of mapping out how to think about a digital motor output. Go and have, check out that paper so I think we spoke about that. So, you know, I think just to make the point we've missed you know, with a low output system so if you know where we'd like to get to is complete point and click like a mouse moving a cursor around the screen and then a click. We have not gotten to that yet. We've got to a low number of clicks. But not we haven't, we haven't solved two dimensional control. So So we've calling our system a synchronous switch because it's kind of built around these discrete key press outputs. But because it's simple and stable and easy to +3
use and work straight away for the patience, we're now building these layers on top and this is just an example where as distinct from, you know, moving the cursor around the screen to make selections of letters, using something like chat GPT or an LLM to start building out predictions of like sentences and phrases. That's context dependent. Our patients love this because they're able to have much more rich conversations and they what they were having before and it's just been a really simple merging of our kind of simple, dependable output with a really high you know, output model that uses LLM. So I think the LLM are going to be this is how LLM 's are going to impact our life. The LLM 's are impacting everyone's what everyone's doing in the world. For us. It's hugely meaningful because it is this great leveler where it gives access to our patients. To really complicated outputs. Okay, so here's one of our patients in he's in New York. This gentleman was told he would have not been with us 10 years ago. He's got ALS. He's had ALS for I think 15 years and he was totally dependent on other people all the time. He can only he can move his eyes a little bit and you can set your same smile at the end of this. This was the first session he turned on he started using the iPhone with his low number low click System. Why this is so meaningful for him is because he has this man has zero privacy. If he ever needs anything someone has to come in and try and interpret what he's looking for. So I'll hit play here. But what you're going to see is him sending these key 
+1
presses to make selections on this app which is going to report pain for him. So this is one of the applications of the system where users are able to navigate their way through, particularly an iPhone you use it on their own Speaker 1
the sound drops off here, but he smiles here at the end. It was a really awesome moment for him and he's now been using this system. So you know we still have we still have like there's a thing down here which we're going to miniaturize and anyway, he's still had to run it through windows. So it still feels a little bit you know, laboratory esque. But the whole system's getting smaller and smaller. And by the time we get to the pivotal trial, it's going to be that what I showed you on that first slide so that was on an iPad. So you know, this is this is another one of our patients using a crosshair to navigate his way through a screen and he's doing some finances here. And then for patients who can oh and then so this is an example of you know, again, using the using the LLM to generate different and then it speaks for him
Speaker 1
I can talk to you with my thoughts on what I don't have when I was going to show with some other demos. So for patients that can still use eye tracking the eye tracking is a really good way to navigate. It sort of solves the two dimensional cursor problem of moving around the screen, but it's not good at clicking. And so the combination of our clicks with the eye tracking gives the users a really beautiful experience and for those that have eye gaze its solves a problem that is with eye tracking. So I think that's going to be the sort of multimodal access so you know it let's say for instance the the vision pro that's coming is really interesting use case because it's got the vision pro needs you to it uses your eye tracking, but then it uses your hand gestures to make selections. So we can very easily replace those hand gestures with outputs directly from the brain and utilize eye tracking. I just I think eye tracking is going to become ubiquitous in our lives. And I were excited about that because we, you know, not many basic for people whose eyes work BCI is not going to do better than eye control. But if you remove the click through the eyes, that's what causes the eyestrain and the headaches. So if you can generate the clicks internally, it's kind of the best of both worlds. So that's kind of what we're preparing and building towards. And then we've been working with Apple we're working with Alexa as well. They're sort of doing some really interesting demos of Alexa voiceless Alexa control as well. So lots of different pathways forward but we've kind of got to stay focused. I just wanted to  show this is our second patient Phil. He has ALS you'll see you'll see him move his hand he still had some degree of movement, which has deteriorated since then, but this was also his first session and he is using eye tracking. Actually you can see the eye tracking bar here. I show this because it shows what it feels like for him to restore control over the computer where he started to lose that. And it's that feeling of autonomy or the agency piece that I was speaking about. You know what it feels like to lose it but getting it back is a really powerful feeling. And this was his reaction in this first session to see the file.
show this is our second patient Phil. He has ALS you'll see you'll see him move his hand he still had some degree of movement, which has deteriorated since then, but this was also his first session and he is using eye tracking. Actually you can see the eye tracking bar here. I show this because it shows what it feels like for him to restore control over the computer where he started to lose that. And it's that feeling of autonomy or the agency piece that I was speaking about. You know what it feels like to lose it but getting it back is a really powerful feeling. And this was his reaction in this first session to see the file.
+1
show this is our second patient Phil. He has ALS you'll see you'll see him move his hand he still had some degree of movement, which has deteriorated since then, but this was also his first session and he is using eye tracking. Actually you can see the eye tracking bar here. I show this because it shows what it feels like for him to restore control over the computer where he started to lose that. And it's that feeling of autonomy or the agency piece that I was speaking about. You know what it feels like to lose it but getting it back is a really powerful feeling. And this was his reaction in this first session to see the file. Speaker 3
Does any old file. Try and stare at it and think about moving for a long time and a sudden zooming in? Yeah, and release. So you made it click your first point, whatever. Okay. So I want you to click on that by staring at it and thinking about moving or planning the movement. Yeah, and then try and relax but right so you open up Word. So it's a combination of zoom and click. Now I want you to open up exactly the same thing open up a blank document for me. But now just start typing whatever you want the time. What are you looking at the time there'll be a W
Unknown Speaker
very, very close. There you go.
Unknown Speaker
Quite well as Walu
Unknown Speaker
is trying to say welcome. Wow, that was that. That's and that's my first attempt. At trying to do that. Yeah, it's amazing
Unknown Speaker
you sort of kept going
Speaker 1
Yeah, 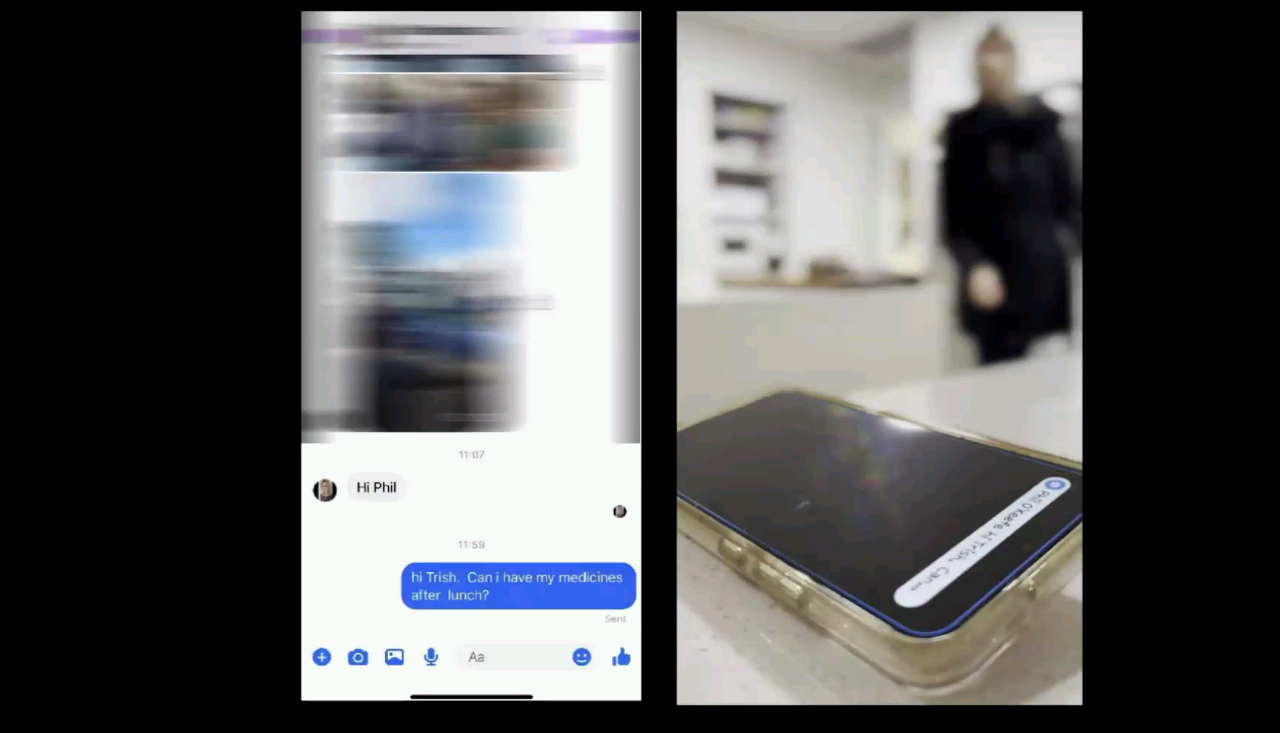
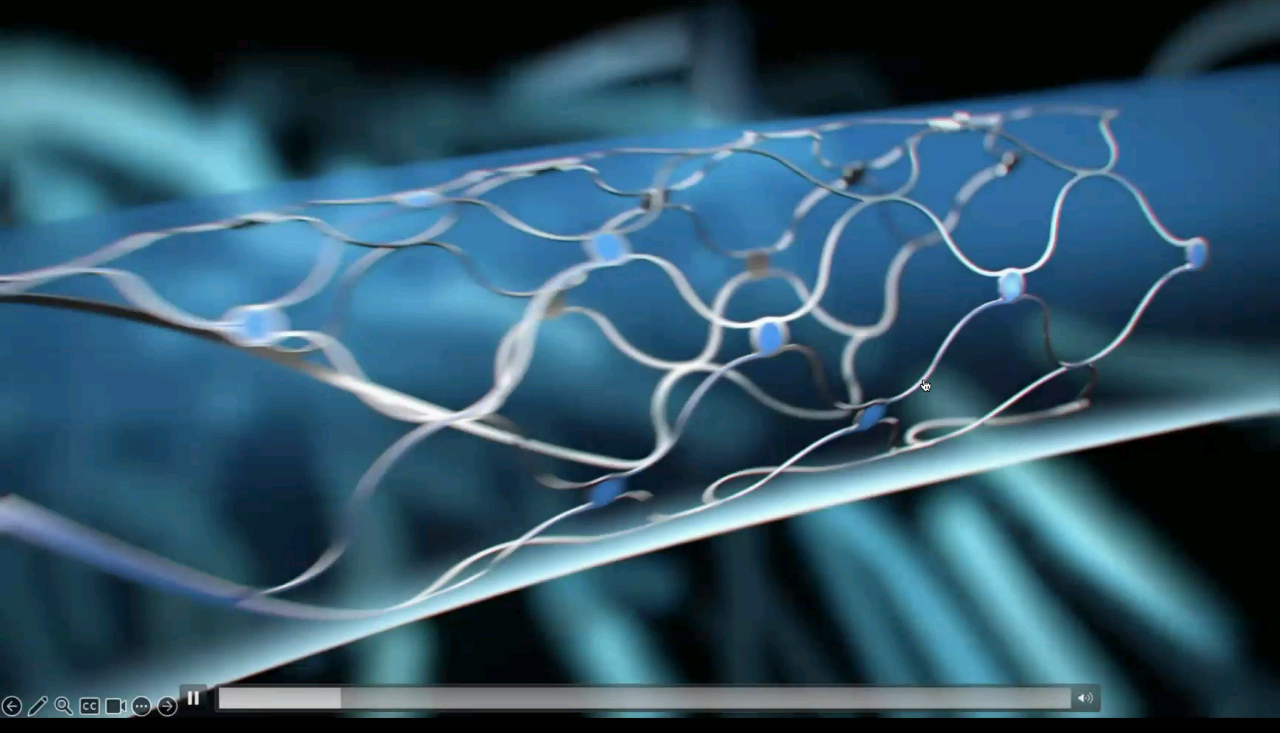
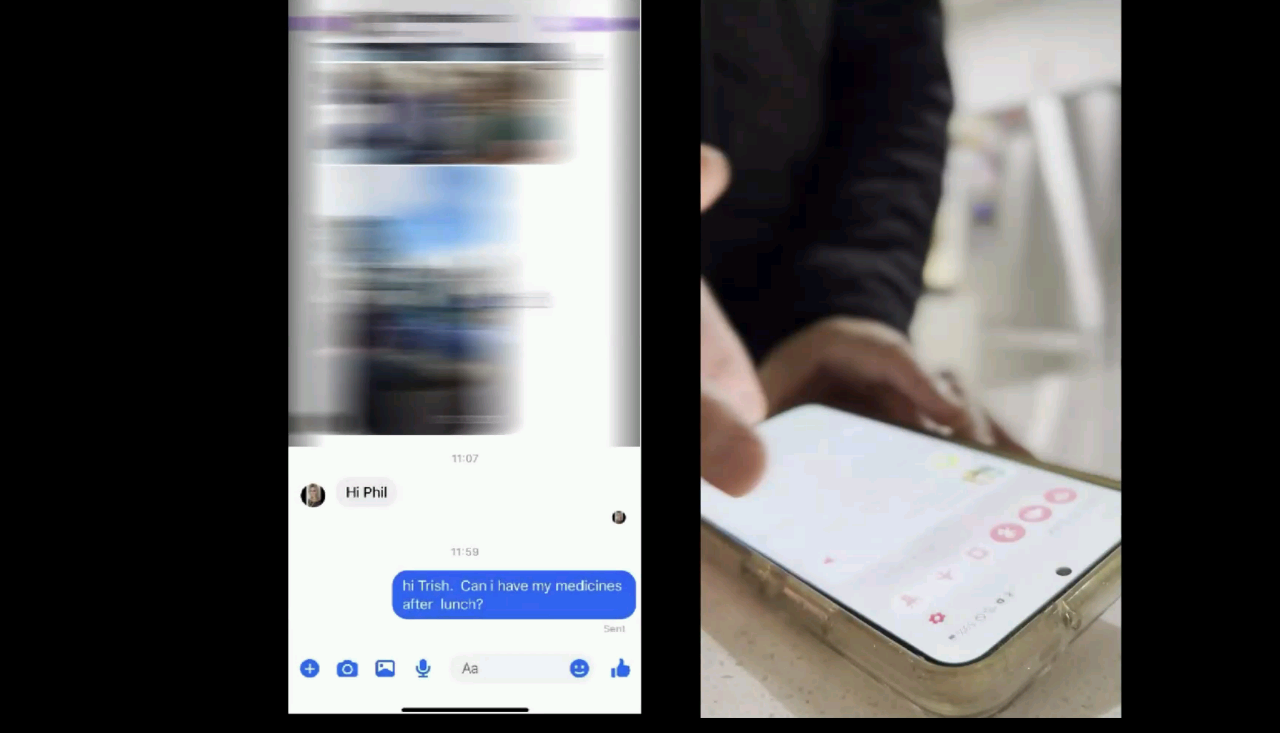 so this is Phil now I just I liked this because we got him on to I think is this messenger. I think it's a messenger on Facebook and that's what him and his wife use and his wife was, you know, normally around and having to you know, keep checking in on him. But once you restore text messaging, the caregiver can actually is emancipated can leave the house can do other things. So, you know, that's the sort of impact on the life that comes with that digital autonomy piece. And I think that's really what we're trying to deliver for our patients. All right, I've really been dribbling on a bit here, so I'm gonna try and get through this. Okay, so this is the concept is that we build a stent. We put those sensors on the stent, it gets incorporated into the wall, it sits in the in the dural venous sinus, the superior sagittal sinus which sits between the left and right motor cortices, and it picks up activity. So you know, you know where we are right now, like the motor cortex runs all the way down here. We're primarily recording activity along here but the vision for us and you know where our technology is heading is into the smaller and smaller blood vessels to get to deeper and deeper regions. But we the risk with research and engineering is that you never you know are satisfied with what you've got, and you keep striving for the next thing, but with class three medical implant, you just have to draw a line in the sand and say, we're starting here. So you know, we know what our constraints are, we kind of know what our system is able to do. And we're
so this is Phil now I just I liked this because we got him on to I think is this messenger. I think it's a messenger on Facebook and that's what him and his wife use and his wife was, you know, normally around and having to you know, keep checking in on him. But once you restore text messaging, the caregiver can actually is emancipated can leave the house can do other things. So, you know, that's the sort of impact on the life that comes with that digital autonomy piece. And I think that's really what we're trying to deliver for our patients. All right, I've really been dribbling on a bit here, so I'm gonna try and get through this. Okay, so this is the concept is that we build a stent. We put those sensors on the stent, it gets incorporated into the wall, it sits in the in the dural venous sinus, the superior sagittal sinus which sits between the left and right motor cortices, and it picks up activity. So you know, you know where we are right now, like the motor cortex runs all the way down here. We're primarily recording activity along here but the vision for us and you know where our technology is heading is into the smaller and smaller blood vessels to get to deeper and deeper regions. But we the risk with research and engineering is that you never you know are satisfied with what you've got, and you keep striving for the next thing, but with class three medical implant, you just have to draw a line in the sand and say, we're starting here. So you know, we know what our constraints are, we kind of know what our system is able to do. And we're 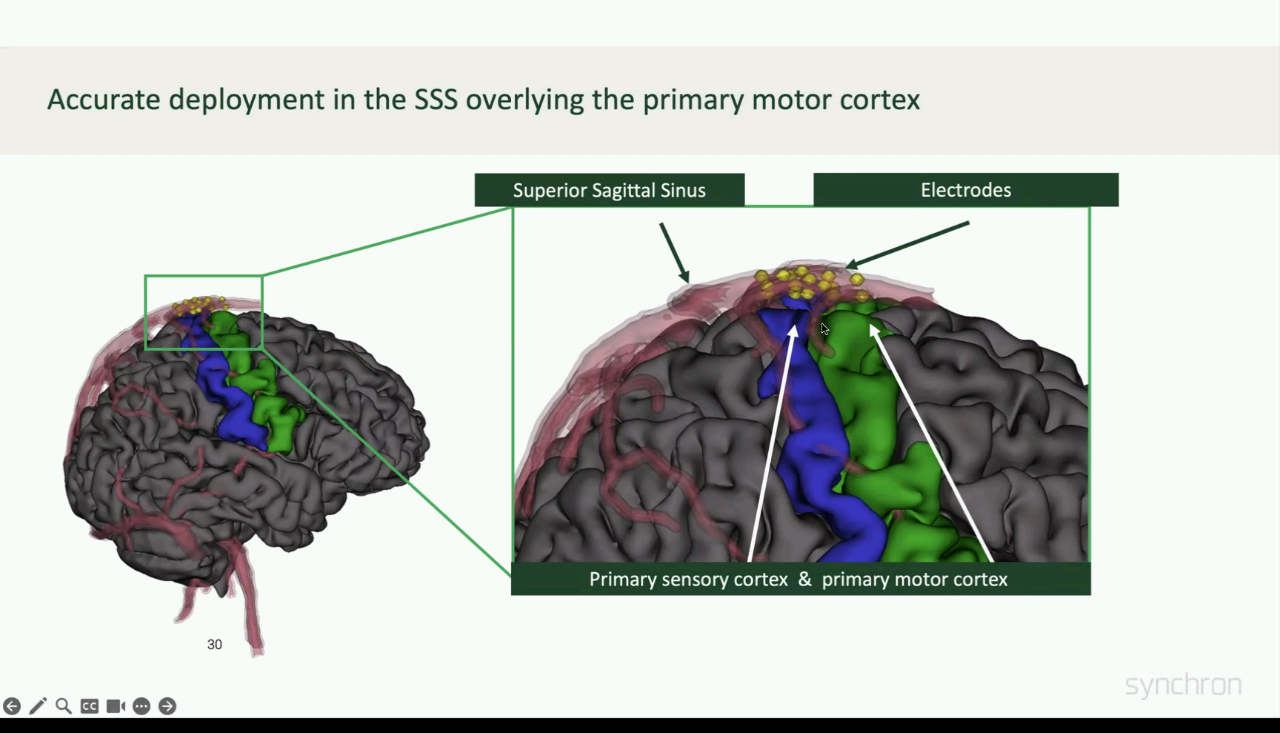
 now building a social software platform around the active activation of activity that we get from this particular region of brain. So I'm stents normally anyway, we there was a big huge manufacturing challenge to create an insulation layer between the two metals layer, that's our sort of secret sauce, which no one's done before. And then, you know, for the physicians during the implants, they have to land the electrode right over the motor cortex. So the targeting that has existed in neurosurgery for functional neurosurgery over a long period of time, it doesn't yet exist for Neuro intervention. So we're having to bring in a lot of the technology to enable brain targeting from within blood vessels which normally you don't have to worry about. Different to the gliosis reaction. I told you about earlier, you have a a reaction, akin to skin scarring, so you have a small layer of scarring that occurs, the device gets incorporated in and then it stops. So it stabilizes and that's really important from a signal perspective because what you have then stays the same when the tissue interface stops changing, which is really important from a from a decoding software
now building a social software platform around the active activation of activity that we get from this particular region of brain. So I'm stents normally anyway, we there was a big huge manufacturing challenge to create an insulation layer between the two metals layer, that's our sort of secret sauce, which no one's done before. And then, you know, for the physicians during the implants, they have to land the electrode right over the motor cortex. So the targeting that has existed in neurosurgery for functional neurosurgery over a long period of time, it doesn't yet exist for Neuro intervention. So we're having to bring in a lot of the technology to enable brain targeting from within blood vessels which normally you don't have to worry about. Different to the gliosis reaction. I told you about earlier, you have a a reaction, akin to skin scarring, so you have a small layer of scarring that occurs, the device gets incorporated in and then it stops. So it stabilizes and that's really important from a signal perspective because what you have then stays the same when the tissue interface stops changing, which is really important from a from a decoding software 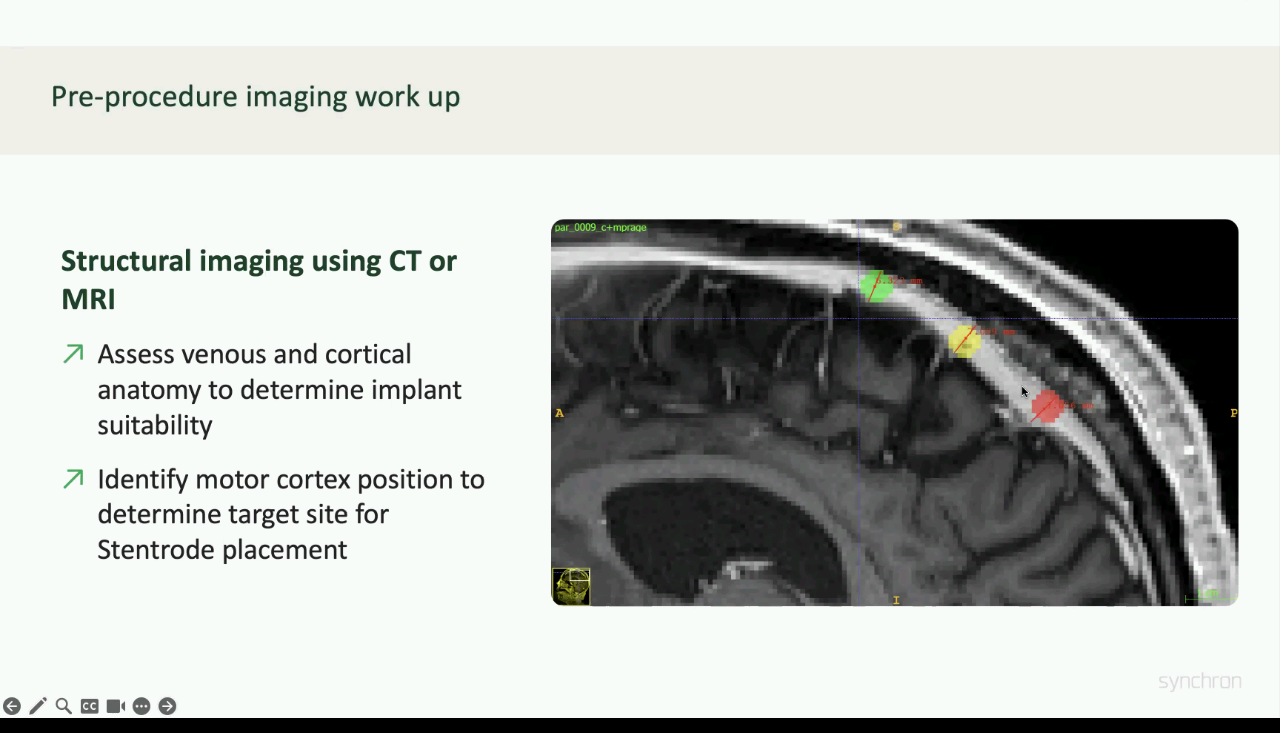
 development perspective. And you know, that's what we are excited about because we think that is a critical feature of our system is stability. So we showed that we published our Australian data in JAMA neurology recently and part of that was showing the stability on bandwidth over a long period of time. You could see it was starting to get a little bit of fluctuation there, but that's on I think, on account of manufacturing challenges that we've had to tighten up on. It Yeah, I mentioned the targeting issue, we have to sort of localize the area of brain relative to the blood vessel and then create an X marks the spot for the physician. This is what a 3d angiogram looks like. Everything's subtracted except for the veins. So we come up here, up here, up here, up here, up here. And then drop it in there. And this is what it looks like in the angio suite. So there's a catheter coming up around here and you can't really see the patient. The physician right now is pushing the device in. The catheter head is coming back. I'm just going to jump forward here you can see the catheter tip is coming back. What you can't see because it's not very visible and X ray yet is the central opening up here kind of like a
development perspective. And you know, that's what we are excited about because we think that is a critical feature of our system is stability. So we showed that we published our Australian data in JAMA neurology recently and part of that was showing the stability on bandwidth over a long period of time. You could see it was starting to get a little bit of fluctuation there, but that's on I think, on account of manufacturing challenges that we've had to tighten up on. It Yeah, I mentioned the targeting issue, we have to sort of localize the area of brain relative to the blood vessel and then create an X marks the spot for the physician. This is what a 3d angiogram looks like. Everything's subtracted except for the veins. So we come up here, up here, up here, up here, up here. And then drop it in there. And this is what it looks like in the angio suite. So there's a catheter coming up around here and you can't really see the patient. The physician right now is pushing the device in. The catheter head is coming back. I'm just going to jump forward here you can see the catheter tip is coming back. What you can't see because it's not very visible and X ray yet is the central opening up here kind of like a
+5
so this is Phil now I just I liked this because we got him on to I think is this messenger. I think it's a messenger on Facebook and that's what him and his wife use and his wife was, you know, normally around and having to you know, keep checking in on him. But once you restore text messaging, the caregiver can actually is emancipated can leave the house can do other things. So, you know, that's the sort of impact on the life that comes with that digital autonomy piece. And I think that's really what we're trying to deliver for our patients. All right, I've really been dribbling on a bit here, so I'm gonna try and get through this. Okay, so this is the concept is that we build a stent. We put those sensors on the stent, it gets incorporated into the wall, it sits in the in the dural venous sinus, the superior sagittal sinus which sits between the left and right motor cortices, and it picks up activity. So you know, you know where we are right now, like the motor cortex runs all the way down here. We're primarily recording activity along here but the vision for us and you know where our technology is heading is into the smaller and smaller blood vessels to get to deeper and deeper regions. But we the risk with research and engineering is that you never you know are satisfied with what you've got, and you keep striving for the next thing, but with class three medical implant, you just have to draw a line in the sand and say, we're starting here. So you know, we know what our constraints are, we kind of know what our system is able to do. And we're 

+2
now building a social software platform around the active activation of activity that we get from this particular region of brain. So I'm stents normally anyway, we there was a big huge manufacturing challenge to create an insulation layer between the two metals layer, that's our sort of secret sauce, which no one's done before. And then, you know, for the physicians during the implants, they have to land the electrode right over the motor cortex. So the targeting that has existed in neurosurgery for functional neurosurgery over a long period of time, it doesn't yet exist for Neuro intervention. So we're having to bring in a lot of the technology to enable brain targeting from within blood vessels which normally you don't have to worry about. Different to the gliosis reaction. I told you about earlier, you have a a reaction, akin to skin scarring, so you have a small layer of scarring that occurs, the device gets incorporated in and then it stops. So it stabilizes and that's really important from a signal perspective because what you have then stays the same when the tissue interface stops changing, which is really important from a from a decoding software +2
development perspective. And you know, that's what we are excited about because we think that is a critical feature of our system is stability. So we showed that we published our Australian data in JAMA neurology recently and part of that was showing the stability on bandwidth over a long period of time. You could see it was starting to get a little bit of fluctuation there, but that's on I think, on account of manufacturing challenges that we've had to tighten up on. It Yeah, I mentioned the targeting issue, we have to sort of localize the area of brain relative to the blood vessel and then create an X marks the spot for the physician. This is what a 3d angiogram looks like. Everything's subtracted except for the veins. So we come up here, up here, up here, up here, up here. And then drop it in there. And this is what it looks like in the angio suite. So there's a catheter coming up around here and you can't really see the patient. The physician right now is pushing the device in. The catheter head is coming back. I'm just going to jump forward here you can see the catheter tip is coming back. What you can't see because it's not very visible and X ray yet is the central opening up here kind of like a Unknown Speaker
flower inside the blood vessel. Why that stopped?
Speaker 1
Anyway, 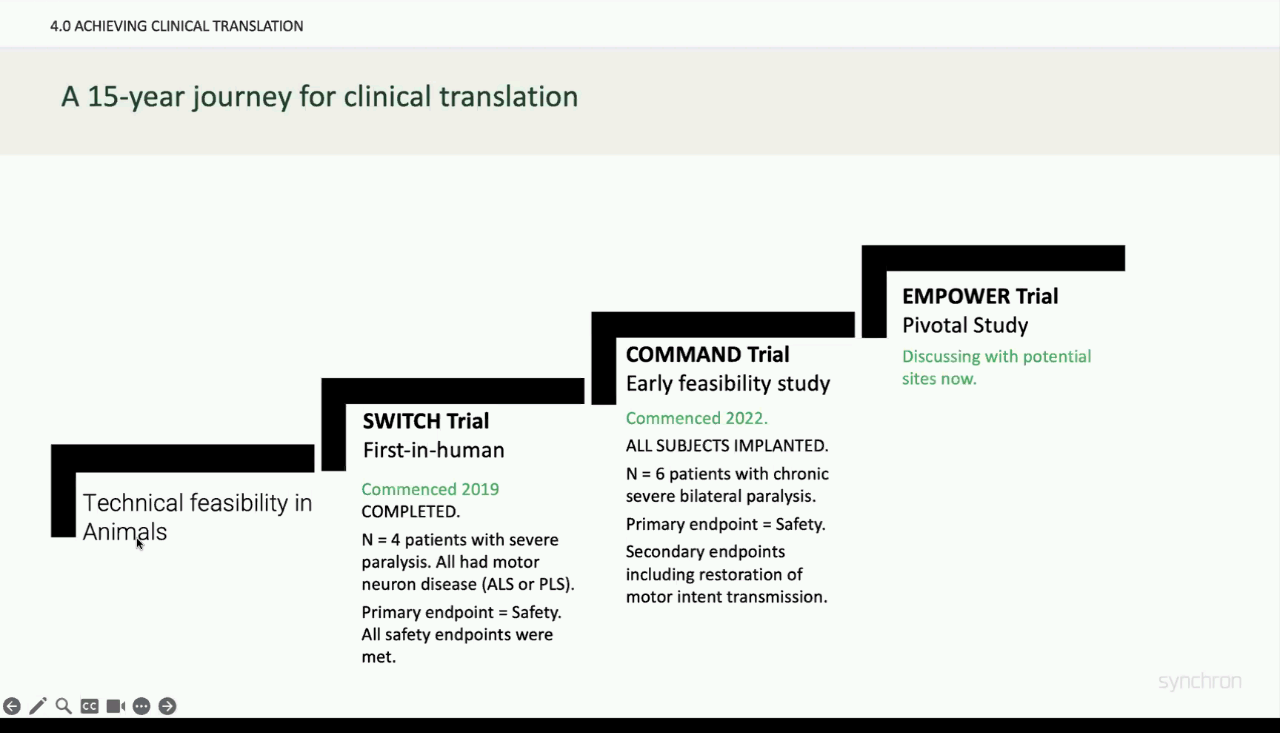
 we'll keep going. And then this is a CAT scan afterwards. That's what the device looks like sitting under the skull inside the brain, kind of inside the folds of the brain not sort of inside the brain itself but inside the sulci within the brain. Okay, almost done. So you know we started out 2012 2016 In in animal preclinical work 2016 and 2017 to 2019 we were preparing for that first inhuman device. We really just published that work 2022 We got our first then we were working on us approvals. So we got our FDA approval for our first study, we launched that. That's now closing up. And then what we're now doing is preparing for our pivotal study and that's going to be I don't know, 2030 sites around the US. I might stop there. So it's been a long journey. We've had lots of support along the way the support early on before we switched into company mode in research mode was so important and you know we wouldn't be here without it. This is a reaction of Graham, our first patient when he was first typing in the sense of achievement and closeness between him and his wife and his wife was able to now leave the house. It's sort of that's what it was all about. And these are the moments that are driving us all to keep working our butts off and make this make this into reality. Thank you and I'd love to take any questions.
we'll keep going. And then this is a CAT scan afterwards. That's what the device looks like sitting under the skull inside the brain, kind of inside the folds of the brain not sort of inside the brain itself but inside the sulci within the brain. Okay, almost done. So you know we started out 2012 2016 In in animal preclinical work 2016 and 2017 to 2019 we were preparing for that first inhuman device. We really just published that work 2022 We got our first then we were working on us approvals. So we got our FDA approval for our first study, we launched that. That's now closing up. And then what we're now doing is preparing for our pivotal study and that's going to be I don't know, 2030 sites around the US. I might stop there. So it's been a long journey. We've had lots of support along the way the support early on before we switched into company mode in research mode was so important and you know we wouldn't be here without it. This is a reaction of Graham, our first patient when he was first typing in the sense of achievement and closeness between him and his wife and his wife was able to now leave the house. It's sort of that's what it was all about. And these are the moments that are driving us all to keep working our butts off and make this make this into reality. Thank you and I'd love to take any questions.
+2
we'll keep going. And then this is a CAT scan afterwards. That's what the device looks like sitting under the skull inside the brain, kind of inside the folds of the brain not sort of inside the brain itself but inside the sulci within the brain. Okay, almost done. So you know we started out 2012 2016 In in animal preclinical work 2016 and 2017 to 2019 we were preparing for that first inhuman device. We really just published that work 2022 We got our first then we were working on us approvals. So we got our FDA approval for our first study, we launched that. That's now closing up. And then what we're now doing is preparing for our pivotal study and that's going to be I don't know, 2030 sites around the US. I might stop there. So it's been a long journey. We've had lots of support along the way the support early on before we switched into company mode in research mode was so important and you know we wouldn't be here without it. This is a reaction of Graham, our first patient when he was first typing in the sense of achievement and closeness between him and his wife and his wife was able to now leave the house. It's sort of that's what it was all about. And these are the moments that are driving us all to keep working our butts off and make this make this into reality. Thank you and I'd love to take any questions. Speaker 2
Great. Thanks. So we're going to that's the main amazing talk. So I've got one question. We were asked over Eventbrite that I'll ask on their behalf if that's okay. So the question was obviously, at the moment, you know, you're particularly targeting motor cortex, what's feasibility for targeting, you know, other functions in the future?
Speaker 1
Yeah. We've got 120 patent applications right now, and they're all they're all kind of in a 20 or so different patent families. So I've been thinking about that question a lot. And the blood vessels go everywhere. There are deep blood vessels, their arteries, their veins there. There's access to all corners. It's just a matter of, you know, and then you can sense or you can stimulate. So, you know, I think I'd broadly characterize what I'm excited about as neuroprosthetics. Monitoring. So like long term monitoring, and I think that's important in things like epilepsy where there's no currently no long term monitoring available for patients if you can do that in a safe way. That can be really impactful. Mapping, I think, I think about mapping is distinct from monitoring because mapping is not an implant. It's a kind of snapshot in time. It's a data representation in brain. I think that's what happened in cardiology with an EP cardiac EP was where interventional cardiology then brought electronics and mapping and then ablation appeared. So now you know, atrial fibrillation can now be treated with a mapping study and then an ablation therapy, I think that is out in front of us for the brain from the blood vessels as well. And then obviously, deep brain stimulation. I think, you know, I think what happened in again, in cardiology, for cardiothoracic, will be similar, and I think patients will choose not to have a craniotomy, if they can avoid it, and I think there are some technical challenges for stimulation, but I'm very excited about endovascular deep brain stimulation.
Unknown Speaker
Cool, cool. Okay, undress, John. Okay.
Speaker 4
To bring it all up, we've got a couple of questions that are maybe a stab at some technical ones. I mean, it's really impressive what this single click can achieve and how you how you map that onto you know what the patients really want. But I'm almost surprised that you can't get more than one dimension, robustly out of even the system as it is let alone if you were to have a longer stent or brand into what limits that. What do you think from the sort of physics of it limits the number of dimensions you can get from the electrode arrangement at the moment?
Speaker 1
We're still hopeful we can get six to eight dimensions, and we've demonstrated up to five dimensions with our system, but you can find that in the Jama neurology paper issue is that the and you know, it's Signal to Noise things it's noise in particular. And it's variability and so, all of these issues around simplicity and stability of use. We've made a decision to focus more on amplifying what we can easily achieve with everyone versus what, you know. We're spending all our time trying to extend the use cases and the it's the stabilities, not there of the system. So
Speaker 4
you'd rather want the patient to robustly know they can always get their click and rather than thinking, you know, the frustration of having something not working that is sort of a three or four dimensional question and see.
Speaker 1
Exactly and it's also about what are you going to build the basis of your clinical medicine around? So we're going to build a system where there's a training capability to keep getting better at this system, but we're actually you know, we've only got 10 patients of data to work with. So we're also have a paucity of data. We have barely even deployed deep learning models yet. We're old. These are all linear decoding classification systems because they just work and they don't need to be trained on. So I think there's there's a lot of excitement about what's out ahead of us, but the kind of pragmatist in me is like well, what what do we need to do to you know, have the lowest bar for clinical meaningfulness and the highest number of patients that we can build a product around?
Unknown Speaker
Amen, I can see you you've got a question or ask your question live.
Speaker 3
Yeah, sure. amazing talk. So two questions slightly, two, quite different. The first is, do patients have to take an A blood thinning medication with your system?
Speaker 1
Yes, so, we have we looked at the literature on transverse sinus stenting for Idiopathic Intracranial hypotension. And we basically did what they do there, which is aspirin for 12 months and clopidogrel for three months. So drill any platelets three months and then aspirin for 12 months, but then they stop. So after 12 months, they're not on anything. Right. Okay. And it's a different question. How do you split your week between clinical work and obviously research and startup work? My wife would wish that I had zero clinical work now, but I'm still holding on to a small amount of coal I'm doing one weekend a month and I only do I don't do any clinic. I just do emergency in your interventional procedures like strokes and ruptured aneurysms. I'll do one weekend, a month and one week, a year of of emergency call. So I've that's kind of I think the lowest it's still because it's such a busy center in the US. I'm still doing about 50 cases a year, which I think is the minimum amount need to sort of stay good enough to treat a family member. That's how I think about it. I don't know if I'm going to keep doing it forever. But I'm I'm so reticent to stop doing clinical medicine because it's just keeps everything grounded and keeps keeps you know, helps. I think helps with that direction on where. Awesome, thank you
Unknown Speaker
okay, great.
Speaker 2
We've got some other questions from the audience. She asked this question from Cindy. Hi, this is one of our neuroscientists said Is there any increased risk of thrombosis from doing stimulation specifically?
Speaker 1
That's a good question. That's a really good question. Yes, there's a there's a dose dependent risk on because you get all sorts of things like heat and tissue agitation with increased stimulation. So there's there's a dose dependent curve on what that looks like. But we know like, we know from for example, deep brain stimulation that uses leads that, you know, whatever is working in DBS in the brain is I think at a level acceptable that wouldn't be causing thrombosis but there is a dose response curve to
Speaker 2
Dorian, Dorian, I see you've written quite a long question in the chat. You want to ask it directly.
Speaker 5
Yes. Can you hear me? Yes. Yeah. Hi, Tom. Nice to meet you. And thanks for the fascinating presentation and also the pioneering work that even the synchrony team are doing. By the way, I'm doing Hachi. I'm the CEO and co founder of Madura a spin out from Imperial College London. We are building the foundational technological foundation ready for the next generation you really implants and we're starting from developing tiny wireless chips and implantable. So my question is really on the term scalability. So I like to have your definition of it. So is it the number of dimensions and or channels? Is it the size of implants, or is the number of patients that can access it? So because I've heard many different definitions, I would like to have yours.
Speaker 1
Yes. So for me the again, this is just a pragmatist talking like the way that we got this far was by hearing what the investors need to hear to invest money into the company to be successful business. Scale scalability that has resonated with our story is not how many electrodes you can get in it's how many patients you can treat. And so for us, I think the the big thing that has been, which we haven't, which is really lucky for us is one of the challenges with BCI in terms of scalability out to patients is what level of hospital infrastructure is needed to deliver the technology. And you know, part of the issue with say the neuropathy system with epilepsy, although there's a range of issues or even Parkinson's disease, deep brain stimulation, part of the issue has been that you need to be usually in a quaternary level neurosurgery center, because it's a long operation with highly skilled open neurosurgeons performing the procedure. With endovascular it's a cath lab, and Cath Lab infrastructure is now exists down to the secondary level hospitals and community level hospitals. And our procedure is quite straightforward. So when I think about scalability, it's how do you deploy this technology at scale to a very large number of people? And for us, it's using a hospital hospital infrastructure that already exists. And there's a million stents and pacemakers being put in on an annual basis in the US now. So, okay,
Unknown Speaker
thank you very much.
Speaker 2
Thank you, and and thank you very much for a great presentation. And there's so much to discuss, and so many of the points you made are really, really important for us in terms of translating technology. There's a couple of questions in the in the chat and one that resonates with what I wanted to ask you as well, which is how did you approach the technical challenges? So you told us that initially, the funding that you got through the academic route was really important. Could you give us an idea of how much of the work initially was engineering and how much was driven by clinical need?
Speaker 1
The early work was still engineering. But, you know, the Nature Biotechnology paper in 2016, we came up with a set of experiments in the animal model that we thought had clinical had correlates to clinical meaningfulness, so I'd still say both, but we had to prove that we could get electrodes into the brain using a blood vessel without a craniotomy, and then we did experiments to show that we could detect signal to noise that we thought would be meaningful enough to move into human clinical translation.
Speaker 2
Thank you. I think it resonates a lot with us the idea that the clinical need was driving you from the earlier stages. And I didn't want to put these words out.
Speaker 1
Even for the preclinical design, you still need to be driven by answering questions that point to a clinical problem. Yeah,
Unknown Speaker
yeah. Thank you. Ashwin, do you wanna go?
Unknown Speaker
Yeah, fascinating talk. Thank you so
Speaker 1
much. reading some of the early work that it's done in animals from Miguel Nicolelis and stuff it seems that he was able to decode motor signals from lots of different places in the brain. How important is being near the paracentral lobule? Have you tried it in other places? Do you still get decoding power? Could we be putting this in a less risky place, for example, more peripherally in the venous system? The answer is we've the safest area is the biggest blood vessel and the biggest blood vessel happens to sit right on top of the parasagittal region of the motor cortex. Part of that is that it has a thick dura, and when you leave the dura go into the surface of the brain into the subarachnoid space. You've got a quite a soft, soft wall venous wall. So when we chose the safest thing first, that was what drove the decision making I think we have to get our system really soft to go into those other regions to get, you know, deeper territories.
Speaker 6
Sorry, I don't know where you're going to ask your question. Yeah, hi, thanks. I wanted to ask if the entire subject transferability is an issue with the central because a lot of papers that I've read on BCI in general, that seems to be a core issue and scaling it to multiple subjects. And I was wondering how you're tackling that with your device.
Speaker 1
Yeah, I mean, I don't know if you saw the talk Illinois. That's kind of what I was talking about. For the majority of the talk is like that's exactly what we're doing is we are the low low key press or low click System works the first session and it works in everyone. And so rather than trying to get to high levels of performance, that's variable across subjects, we are choosing something that everyone can do very easily and then building a system around that. So that gets to the exact heart of how we're designing.
Speaker 6
Okay, thank you so much. Sorry, if I can follow up on that. Just to have one more question more about your journey as opposed to your product. I was wondering when you were in the process of sort of building your team, since you come from a medical academic background, how did you source the tech knowledge for this venture and how did you decide who you needed for that as well?
Speaker 1
I think we'll need to meet at the pub over a few beers to discuss that. But it was very hard and I had to figure out a lot of it myself and I had to hire people who could do a lot of different things and be problem solvers and work in areas that you know nothing about and find people who know the answer, but it's, you know, that's a there's no easy answer to that. Other than you've got to solve the most critical things first and find people that can wear lots of different hats and exist in chaos and in exactitude.
Unknown Speaker
Thank you.
Speaker 2
Thanks. I think we're out of time. So should we have one last question? I suggest to undress you want to ask the last question
Speaker 4
it's very kind Well, it's maybe the most critical so maybe not the best read but critical to your work but your your highlight this beautiful paper from the Grande from from a while ago now. That really works very well for that patient. The why is no Why isn't that why hasn't that been rolled out more widely? Why is it not a routine clinical term?
Speaker 1
That's a great question, Andreas. I mean, I think if you're gonna if you ask Nick Ramsey that question the you know, another way to phrase the question is, why didn't you form a company around that technology and do it and the answer is, it's really hard to do. They borrowed a Medtronic system, Medtronic have chosen not to pursue it. It wasn't exactly fit for purpose. Medtronic would have had to have invested, it takes about $150 million to get pockets. So, you know, you can ask Nick Ramsey, why didn't you go and raise $150 million? It's really hard to do. He would have had to have give up his academic career and start building a team and go all in on that and take a risk on whether it was going to work but I think it's a really good question why and I asked the question, I'm like, why is this such a big focus in BCI on these super high channel count systems when there's this huge gap with what the actual patient need is like, I'm, you know, I asked this question a lot. And I'm, it just makes me push on, like being very happy to live in this lower, you know, fidelity world because it has such potential meaningfulness to the system and not play this tech Race game that's going on.
Speaker 4
It just seems odd that Medtronic, for example, wasn't interested in following and following on is it just too difficult for them more than enough to figure out what's the use case and how to convince the the, as you said, ensures that this is actually going to restore independence? Does that make sense?
Speaker 1
And Tronic Boston, j&j Abbott have they? Have a bad track record for innovation, they only purchase companies and so they sit back and they wait, and then they wait until you've almost got all the way through and then they make a purchase. So I think if they're going to do it, they would want to sort of purchase another company rather than do it themselves. But I don't want to sell to them because I think they'll screw it up. So I'm not going to do
Unknown Speaker
you agree? Thank you very much.
Speaker 2
Well, remains to say, Tom, thank you so much for making time to talk to us. I mean, I think we think you know, speak for everyone said what you're doing is amazing, and it's been great to have have a chance to hear about it from you directly. For everyone else do follow the impact near attack, Twitter, which is at impact neurotech for more talks in a series, and
Speaker 1
like, hey, we'll just gonna say my email was just tom@syncron.com If anyone wants to reach out over any other questions or anything else, I'm happy to speak to anyone. Thomas syncron.com. Cool. All right. Thank
Speaker 4
you so much, John. Really brilliant. Thank you. Thank you. Very much for having me. Well, thanks. John.