Loading...
BRIGHT Institute webinar
Unknown Speaker
Address You
Unknown Speaker
all right, we're going to get started. Welcome everyone. I am Lorien abroms, Professor of Health Communication at the George Washington University, the Milken Institute, School of Public Health, and I'm also the co director of the bright Institute. And welcome to today's webinar from the bright Institute on the topic of AI for social and behavioral change. We're going to have three wonderful presenters today, and I'll go ahead and introduce the three presenters, and they'll present, and then we will take questions and have a great discussion on AI and health behavior change. And if you have questions during the presentations, please put them in the chat, and hopefully there'll be time and we'll get to them all by the end. Okay, so our first presenter today is Dr Jordan Boyd Graber and Dr gray boy Graber is an associate professor at the University of Maryland's computer science department and language Science Center, and an affiliate Professor of the School of Information. Jordan is focused on the applications of artificial intelligence in language based settings such as question answering and information triage, as well as building evaluations for these models and understanding the relative human versus computer abilities, very important and relevant in this time. And he's going to be talking about an LLM chatbot that he has created for maternal health. Our second presenter is Dr Doug Evans, and I'm going to go ahead and just introduce all three, and then we'll we'll start off with Jordan. Our second presenter is Dr Doug Evans. He's a professor of Communication and global health in the milk Institute School of Public Health at the George Washington University. And Dr Evans work focuses on the translation of communication and marketing strategies, primarily digital media based methodologies, into interventions to promote adoption of health behaviors and avoidance of health risk behaviors. And he's going to be talking about his work with AI for digital intervention delivery and evaluation. And then finally, our third presenter is Katerina bots you and Katerina is a communications professional with a passion for human humanitarian work and a specific focus on serving underprivileged populations. She currently works with the World Health Organization on various digital projects, leveraging technology to make a positive impact in the world and help people live longer, healthier lives. She's worked as a communication specialist with the United Nations Office at Geneva, the International Telecommunications Union, and the United Nations Institute for Disarmament Research. And she'll be talking about the WHO chatbot called Sarah. And with that, I'd like to turn it over to Jordan to present on on maternal health. Go ahead, Jordan,
Unknown Speaker
yes, 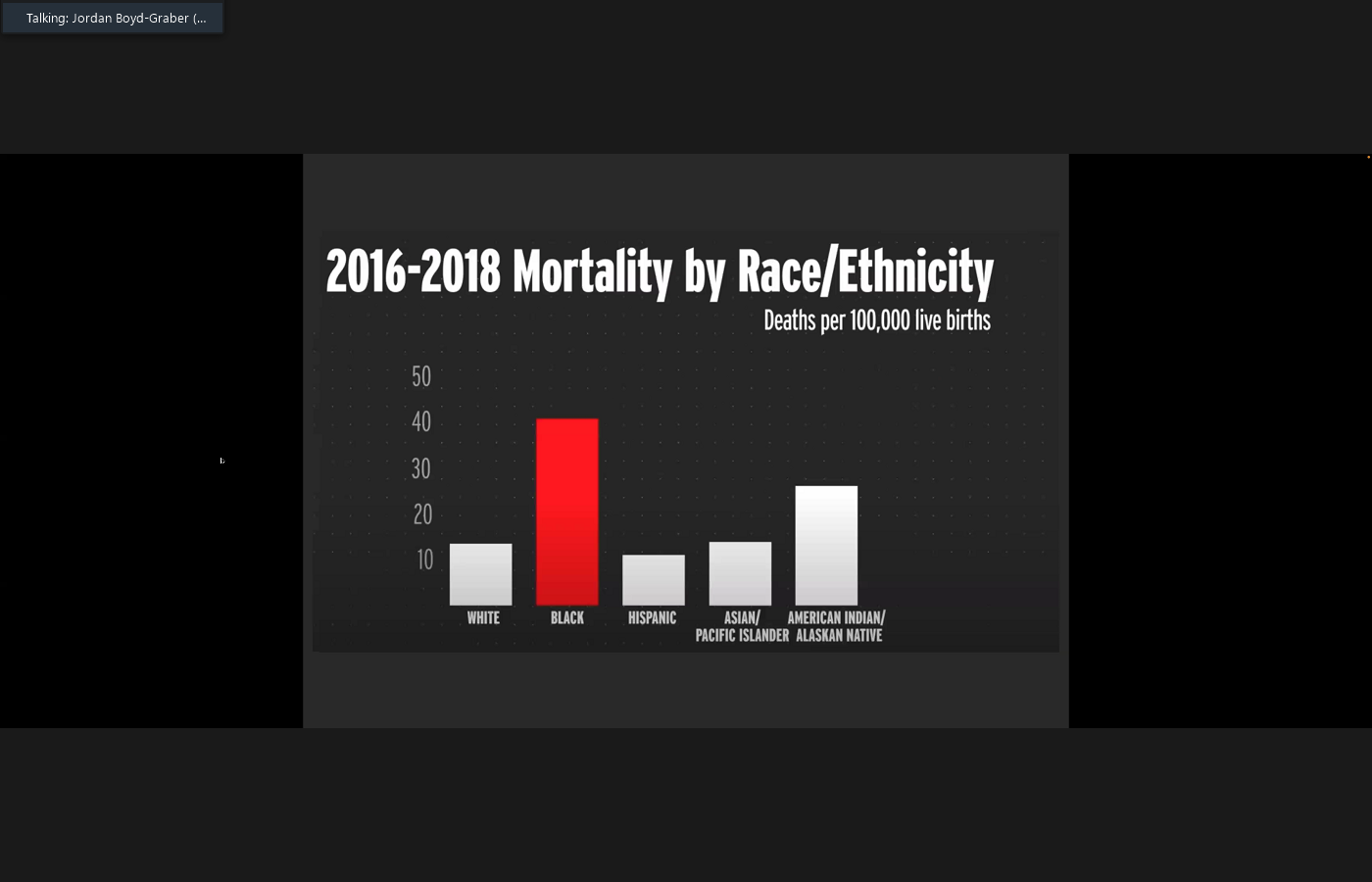
 thank you so much for having me. It's a pleasure to be here. Yeah. So let me first say that this is a collaboration with a bunch of wonderful people. So Neha is a graduate student in computer science who did most of the work in creating the agent. And then there are a lot of collaborators in public health and statistics at the University of Maryland who actually did the hard work of getting this out into the field and getting people to actually use it. So the motivation for our work is that maternal outcomes in the United States aren't that great compared to our peer countries, and a lot of this is attributable to disparate outcomes, particularly for underserved minorities. And there are many things that go into this, and Doug can probably talk about this better than I can, but one part of this is access to information, and we are trying to address that with a chat bot that my collaborators named Rosie. And the idea is that we want to have an intervention where we provide mothers, new and expectant others with vetted, trustworthy information, and then measure how that changes health outcomes. And
thank you so much for having me. It's a pleasure to be here. Yeah. So let me first say that this is a collaboration with a bunch of wonderful people. So Neha is a graduate student in computer science who did most of the work in creating the agent. And then there are a lot of collaborators in public health and statistics at the University of Maryland who actually did the hard work of getting this out into the field and getting people to actually use it. So the motivation for our work is that maternal outcomes in the United States aren't that great compared to our peer countries, and a lot of this is attributable to disparate outcomes, particularly for underserved minorities. And there are many things that go into this, and Doug can probably talk about this better than I can, but one part of this is access to information, and we are trying to address that with a chat bot that my collaborators named Rosie. And the idea is that we want to have an intervention where we provide mothers, new and expectant others with vetted, trustworthy information, and then measure how that changes health outcomes. And  I won't talk about this today. If people want to talk about this in the Q and A, we can, but we're also doing this bilingually, which presents some really interesting challenges, because a lot of the trusted information in Spanish isn't coming from the United States, but coming from other places. And so how do you actually deal with this and give consistent answers to questions in both English and Spanish? And so we have the system. It's out there. It's being deployed. People can go on their smartphone ask questions and then get answers back, but the very focus thing that I want to talk about today is that many of these questions have presuppositions, and so a presupposition is when you ask a question, but you are asserting something to be true, and sometimes these presuppositions are false. And so in the Natural Language Processing literature, there are a lot of examples of this, like what linguists invented the light bulb, or when did Da Vinci paint the Sistine Chapel? And so these are kind of silly examples, but a problem is is that artificial intelligence basically pretends like it's doing an improv skit and rolls with
I won't talk about this today. If people want to talk about this in the Q and A, we can, but we're also doing this bilingually, which presents some really interesting challenges, because a lot of the trusted information in Spanish isn't coming from the United States, but coming from other places. And so how do you actually deal with this and give consistent answers to questions in both English and Spanish? And so we have the system. It's out there. It's being deployed. People can go on their smartphone ask questions and then get answers back, but the very focus thing that I want to talk about today is that many of these questions have presuppositions, and so a presupposition is when you ask a question, but you are asserting something to be true, and sometimes these presuppositions are false. And so in the Natural Language Processing literature, there are a lot of examples of this, like what linguists invented the light bulb, or when did Da Vinci paint the Sistine Chapel? And so these are kind of silly examples, but a problem is is that artificial intelligence basically pretends like it's doing an improv skit and rolls with  this. It is so accommodating to the desires of the person asking the question that it basically assumes whatever the question says is true and then creates an answer predicated on that. And so these kind of silly examples, like linguists and light bulbs and Renaissance painters are fun, but sometimes this is really serious business. And so maternal health is one example where this could be sensitive and important. Other things could be like asking about taxes or money or laws or immigration. And so if our AI systems kind of just roll with the punches and assume these things are true, this could lead to bad outcomes. And if you think about what's happening in a health context, a lot of times, these presuppositions could reflect misconceptions or false information that people have internalized. And so for example, if you take a look at the question, when should I give my baby fever reducing meds after shots, this can mean that the person believes that you can give babies fever reducing medications, that receiving shots can cause fever, that I should give my baby fever reducing medicines after a vaccine, or that there's some interval Between which you need to give medicines after a shot. And some of these are true, some of these are not. And if you ask this sort of question to a doctor, I think a our idealized version of what a doctor should do would be that they would address the presuppositions that are true, maybe reinforce the ones that are true, and maybe combat the ones that are false, or maybe probe a little bit. Why do you ask that, rather than just trying to answer the question as directly as possible? So this is our kind of big picture goal, and
this. It is so accommodating to the desires of the person asking the question that it basically assumes whatever the question says is true and then creates an answer predicated on that. And so these kind of silly examples, like linguists and light bulbs and Renaissance painters are fun, but sometimes this is really serious business. And so maternal health is one example where this could be sensitive and important. Other things could be like asking about taxes or money or laws or immigration. And so if our AI systems kind of just roll with the punches and assume these things are true, this could lead to bad outcomes. And if you think about what's happening in a health context, a lot of times, these presuppositions could reflect misconceptions or false information that people have internalized. And so for example, if you take a look at the question, when should I give my baby fever reducing meds after shots, this can mean that the person believes that you can give babies fever reducing medications, that receiving shots can cause fever, that I should give my baby fever reducing medicines after a vaccine, or that there's some interval Between which you need to give medicines after a shot. And some of these are true, some of these are not. And if you ask this sort of question to a doctor, I think a our idealized version of what a doctor should do would be that they would address the presuppositions that are true, maybe reinforce the ones that are true, and maybe combat the ones that are false, or maybe probe a little bit. Why do you ask that, rather than just trying to answer the question as directly as possible? So this is our kind of big picture goal, and 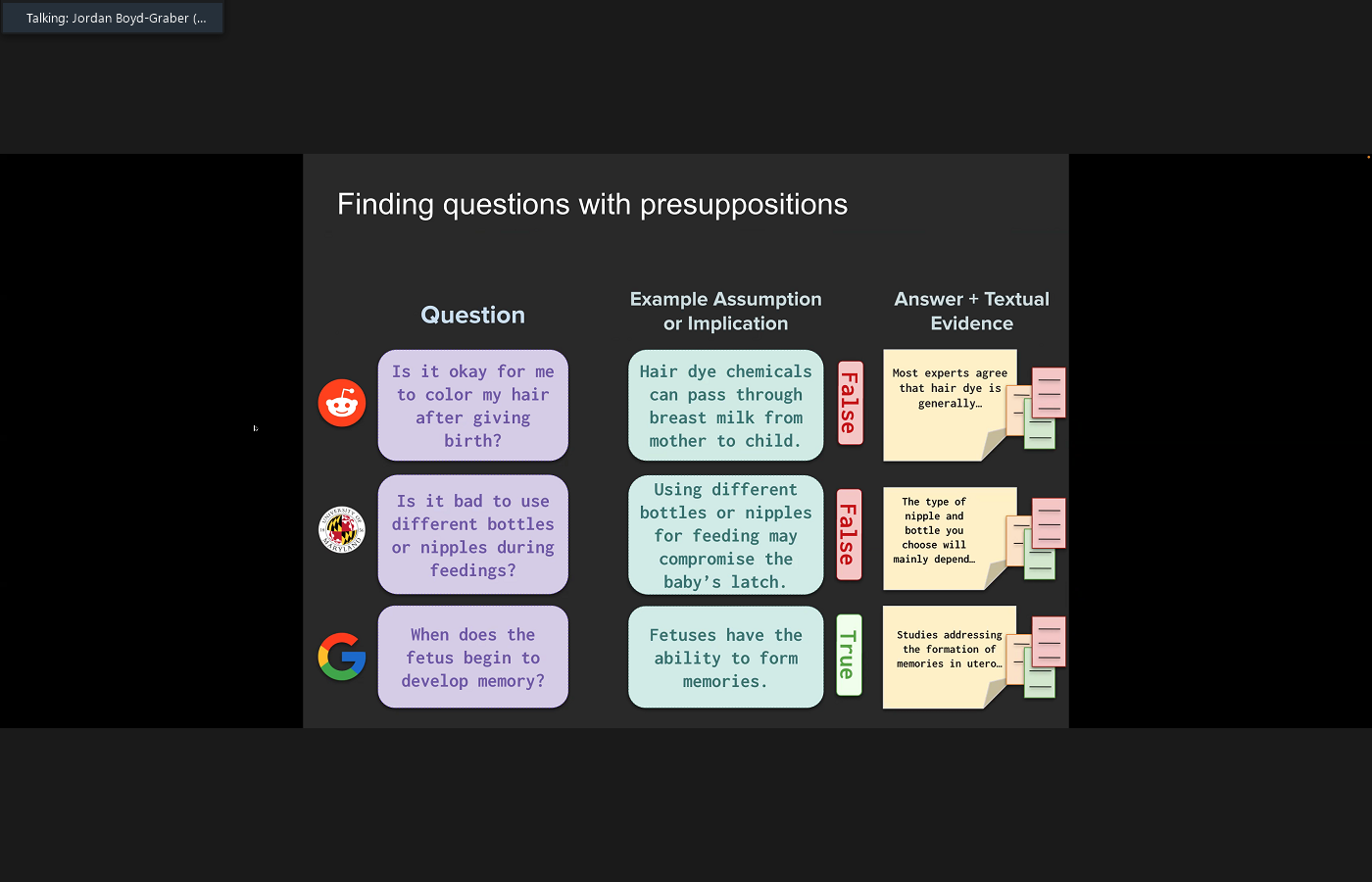
 this is still very much a work in progress. And so if people have ideas or more examples or more use cases that they think would be interesting to look at, we are certainly in all ears. Okay, so to try to address this, what we did is we tried to find a bunch of these maternal health questions that have potentially presuppositions from Reddit, from our own data, interactions with people using the Chatbot, and from the Google resource natural questions. We then extracted the presuppositions in these data, and then we labeled those presuppositions as true or false with public health experts, and then we crafted what we thought would be reasonable answers to those questions. And looking at the data, there are a lot of inferences that can be drawn from questions, so about fivefold or between four and fivefold inferences based on the number of questions, and of those inferences anywhere from a fifth to a third are false. So this is kind of concerning. So this kind of gave us a further boost to our mission of trying to create a question answering system that can address these false inferences. And so I won't go
this is still very much a work in progress. And so if people have ideas or more examples or more use cases that they think would be interesting to look at, we are certainly in all ears. Okay, so to try to address this, what we did is we tried to find a bunch of these maternal health questions that have potentially presuppositions from Reddit, from our own data, interactions with people using the Chatbot, and from the Google resource natural questions. We then extracted the presuppositions in these data, and then we labeled those presuppositions as true or false with public health experts, and then we crafted what we thought would be reasonable answers to those questions. And looking at the data, there are a lot of inferences that can be drawn from questions, so about fivefold or between four and fivefold inferences based on the number of questions, and of those inferences anywhere from a fifth to a third are false. So this is kind of concerning. So this kind of gave us a further boost to our mission of trying to create a question answering system that can address these false inferences. And so I won't go 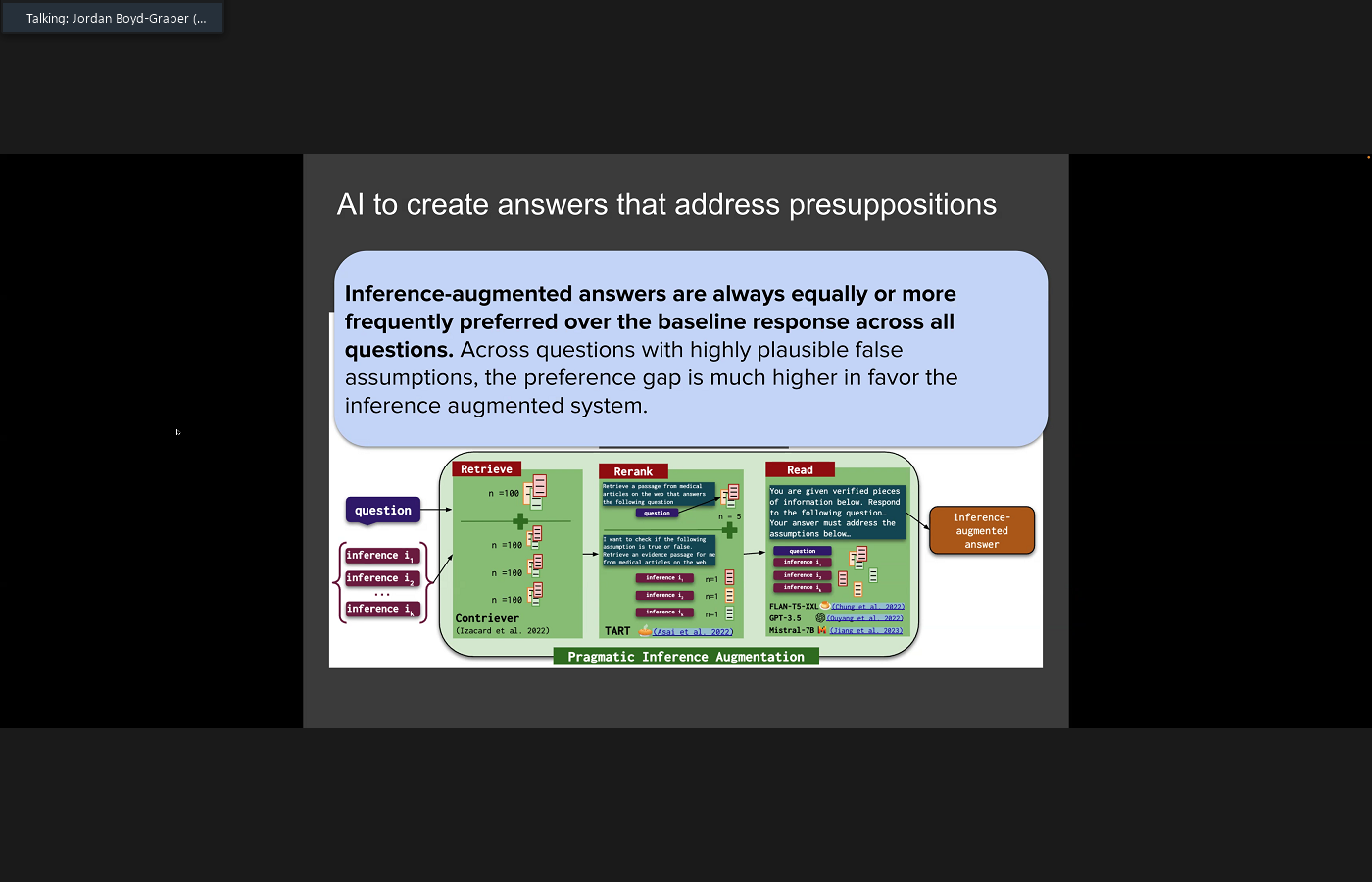
 into the technical details here, but the basic pipeline that we use is we have a system that tries to look at the possible false inferences that could be drawn from a question. Address those false inferences by retrieving targeted information that could either support or refute the false inferences and then ask the abroms engineering a system to answer the underlying question and also to address any of the false inferences that were in the question. We then did a study to check how people like the questions that address the presuppositions and when we added in the responses to the presuppositions, people liked the answers about as much as quote, unquote, normal questions, but the preferences towards these answers increased dramatically when there were plausible inferences that could be drawn. And so this is something that we're continuing to work on to figure out. Well, maybe we shouldn't address all of the possible inferences, but just focus on the ones that are highly probable or the most important. So this is what we're working on right now, and as I wrap up and what I hope we can talk about going forward. I think this is a sign that AI should not be one size fits all, and that's kind of the way that it's been presented right now, because you have a bunch of companies trying to offer a commoditized API to access to artificial intelligence as a service, and that really isn't the best model, because people do need precise, targeted answers, but we don't have that because our data aren't ready. We need data sets that reflect who is asking the question. We need evaluations that reflect user desires. And because we don't have the data, our methods aren't ready either, and so we need alternatives to reinforcement learning with human feedback that take into account who is asking the question. What the question is about. Should it be tailored? And personally, I think there are a lot of tools from psychology, like item response theory, that can help us do this. And because AI doesn't look like this, our policy isn't ready either, and this isn't my metier, and so I think everyone here knows about this at a greater depth than I do, but we also need policy to reflect this. Need to balance privacy and personalization, and that's going to be the next challenge. And so with that, I will stop sharing and looking forward to hearing from everyone else.
into the technical details here, but the basic pipeline that we use is we have a system that tries to look at the possible false inferences that could be drawn from a question. Address those false inferences by retrieving targeted information that could either support or refute the false inferences and then ask the abroms engineering a system to answer the underlying question and also to address any of the false inferences that were in the question. We then did a study to check how people like the questions that address the presuppositions and when we added in the responses to the presuppositions, people liked the answers about as much as quote, unquote, normal questions, but the preferences towards these answers increased dramatically when there were plausible inferences that could be drawn. And so this is something that we're continuing to work on to figure out. Well, maybe we shouldn't address all of the possible inferences, but just focus on the ones that are highly probable or the most important. So this is what we're working on right now, and as I wrap up and what I hope we can talk about going forward. I think this is a sign that AI should not be one size fits all, and that's kind of the way that it's been presented right now, because you have a bunch of companies trying to offer a commoditized API to access to artificial intelligence as a service, and that really isn't the best model, because people do need precise, targeted answers, but we don't have that because our data aren't ready. We need data sets that reflect who is asking the question. We need evaluations that reflect user desires. And because we don't have the data, our methods aren't ready either, and so we need alternatives to reinforcement learning with human feedback that take into account who is asking the question. What the question is about. Should it be tailored? And personally, I think there are a lot of tools from psychology, like item response theory, that can help us do this. And because AI doesn't look like this, our policy isn't ready either, and this isn't my metier, and so I think everyone here knows about this at a greater depth than I do, but we also need policy to reflect this. Need to balance privacy and personalization, and that's going to be the next challenge. And so with that, I will stop sharing and looking forward to hearing from everyone else.
+2
thank you so much for having me. It's a pleasure to be here. Yeah. So let me first say that this is a collaboration with a bunch of wonderful people. So Neha is a graduate student in computer science who did most of the work in creating the agent. And then there are a lot of collaborators in public health and statistics at the University of Maryland who actually did the hard work of getting this out into the field and getting people to actually use it. So the motivation for our work is that maternal outcomes in the United States aren't that great compared to our peer countries, and a lot of this is attributable to disparate outcomes, particularly for underserved minorities. And there are many things that go into this, and Doug can probably talk about this better than I can, but one part of this is access to information, and we are trying to address that with a chat bot that my collaborators named Rosie. And the idea is that we want to have an intervention where we provide mothers, new and expectant others with vetted, trustworthy information, and then measure how that changes health outcomes. And +1
I won't talk about this today. If people want to talk about this in the Q and A, we can, but we're also doing this bilingually, which presents some really interesting challenges, because a lot of the trusted information in Spanish isn't coming from the United States, but coming from other places. And so how do you actually deal with this and give consistent answers to questions in both English and Spanish? And so we have the system. It's out there. It's being deployed. People can go on their smartphone ask questions and then get answers back, but the very focus thing that I want to talk about today is that many of these questions have presuppositions, and so a presupposition is when you ask a question, but you are asserting something to be true, and sometimes these presuppositions are false. And so in the Natural Language Processing literature, there are a lot of examples of this, like what linguists invented the light bulb, or when did Da Vinci paint the Sistine Chapel? And so these are kind of silly examples, but a problem is is that artificial intelligence basically pretends like it's doing an improv skit and rolls with +1
this. It is so accommodating to the desires of the person asking the question that it basically assumes whatever the question says is true and then creates an answer predicated on that. And so these kind of silly examples, like linguists and light bulbs and Renaissance painters are fun, but sometimes this is really serious business. And so maternal health is one example where this could be sensitive and important. Other things could be like asking about taxes or money or laws or immigration. And so if our AI systems kind of just roll with the punches and assume these things are true, this could lead to bad outcomes. And if you think about what's happening in a health context, a lot of times, these presuppositions could reflect misconceptions or false information that people have internalized. And so for example, if you take a look at the question, when should I give my baby fever reducing meds after shots, this can mean that the person believes that you can give babies fever reducing medications, that receiving shots can cause fever, that I should give my baby fever reducing medicines after a vaccine, or that there's some interval Between which you need to give medicines after a shot. And some of these are true, some of these are not. And if you ask this sort of question to a doctor, I think a our idealized version of what a doctor should do would be that they would address the presuppositions that are true, maybe reinforce the ones that are true, and maybe combat the ones that are false, or maybe probe a little bit. Why do you ask that, rather than just trying to answer the question as directly as possible? So this is our kind of big picture goal, and +2
this is still very much a work in progress. And so if people have ideas or more examples or more use cases that they think would be interesting to look at, we are certainly in all ears. Okay, so to try to address this, what we did is we tried to find a bunch of these maternal health questions that have potentially presuppositions from Reddit, from our own data, interactions with people using the Chatbot, and from the Google resource natural questions. We then extracted the presuppositions in these data, and then we labeled those presuppositions as true or false with public health experts, and then we crafted what we thought would be reasonable answers to those questions. And looking at the data, there are a lot of inferences that can be drawn from questions, so about fivefold or between four and fivefold inferences based on the number of questions, and of those inferences anywhere from a fifth to a third are false. So this is kind of concerning. So this kind of gave us a further boost to our mission of trying to create a question answering system that can address these false inferences. And so I won't go +2
into the technical details here, but the basic pipeline that we use is we have a system that tries to look at the possible false inferences that could be drawn from a question. Address those false inferences by retrieving targeted information that could either support or refute the false inferences and then ask the abroms engineering a system to answer the underlying question and also to address any of the false inferences that were in the question. We then did a study to check how people like the questions that address the presuppositions and when we added in the responses to the presuppositions, people liked the answers about as much as quote, unquote, normal questions, but the preferences towards these answers increased dramatically when there were plausible inferences that could be drawn. And so this is something that we're continuing to work on to figure out. Well, maybe we shouldn't address all of the possible inferences, but just focus on the ones that are highly probable or the most important. So this is what we're working on right now, and as I wrap up and what I hope we can talk about going forward. I think this is a sign that AI should not be one size fits all, and that's kind of the way that it's been presented right now, because you have a bunch of companies trying to offer a commoditized API to access to artificial intelligence as a service, and that really isn't the best model, because people do need precise, targeted answers, but we don't have that because our data aren't ready. We need data sets that reflect who is asking the question. We need evaluations that reflect user desires. And because we don't have the data, our methods aren't ready either, and so we need alternatives to reinforcement learning with human feedback that take into account who is asking the question. What the question is about. Should it be tailored? And personally, I think there are a lot of tools from psychology, like item response theory, that can help us do this. And because AI doesn't look like this, our policy isn't ready either, and this isn't my metier, and so I think everyone here knows about this at a greater depth than I do, but we also need policy to reflect this. Need to balance privacy and personalization, and that's going to be the next challenge. And so with that, I will stop sharing and looking forward to hearing from everyone else. Unknown Speaker
Ray, thank you so much. Lots of questions, but we'll hold them until we go through all three of our presenters. Our next presenter is Dr Doug Evans,
Speaker 1
thank 
 you very much. Let me share my screen. Right place here. Give me a second. Hey, hopefully you can see that. Yep, all right, great. Well, thank you all very much. I am going to present on my work on social and behavioral change using AI. And let me just start off by talking broadly about the work that we do here at the bright Institute at GW. So I view using the use of AI for social and behavioral change as falling within the broader field of digital health interventions, or DHS, as they've been defined in the literature. And what I mean by that are basically any kind of program intervention campaign aimed at changing specific behaviors in a population, using digital platforms for the delivery of that intervention and also research to evaluate the effectiveness of those kinds of programs. But a big question that we talked about in a paper a couple of years ago is, how effective are these programs, and under what conditions do they work? They don't necessarily work under all conditions, and we need to understand that context much better than we do now. So AI can definitely be used for social good. There's a lot of discussion out in the media and many areas of literature that talk about all the negatives of AI, but it's definitely the case that AI can be a major force for social good. The McKenzie Institute, just as an example, tried to kind of categorize this idea a few years ago, and they identified these 10 domains of areas in which AI has been shown to be affected to at least a certain extent, in promoting pro social causes and goods. So economic empowerment, education, infrastructure, public and social sector factors, combating false news or polarization, potentially, although, of course, AI can also create those problems. So it's clear that AI can be used for social good, and we have a lot of use cases that are starting to be built up. We need to understand those use cases and be able to draw inferences from them to more effectively design programs using AI in the future. One way that this has been used is in AI marketing, which would be leveraging AI tools and methods such as large language models, to basically develop insights around I'll use the term consumer, but you could also
you very much. Let me share my screen. Right place here. Give me a second. Hey, hopefully you can see that. Yep, all right, great. Well, thank you all very much. I am going to present on my work on social and behavioral change using AI. And let me just start off by talking broadly about the work that we do here at the bright Institute at GW. So I view using the use of AI for social and behavioral change as falling within the broader field of digital health interventions, or DHS, as they've been defined in the literature. And what I mean by that are basically any kind of program intervention campaign aimed at changing specific behaviors in a population, using digital platforms for the delivery of that intervention and also research to evaluate the effectiveness of those kinds of programs. But a big question that we talked about in a paper a couple of years ago is, how effective are these programs, and under what conditions do they work? They don't necessarily work under all conditions, and we need to understand that context much better than we do now. So AI can definitely be used for social good. There's a lot of discussion out in the media and many areas of literature that talk about all the negatives of AI, but it's definitely the case that AI can be a major force for social good. The McKenzie Institute, just as an example, tried to kind of categorize this idea a few years ago, and they identified these 10 domains of areas in which AI has been shown to be affected to at least a certain extent, in promoting pro social causes and goods. So economic empowerment, education, infrastructure, public and social sector factors, combating false news or polarization, potentially, although, of course, AI can also create those problems. So it's clear that AI can be used for social good, and we have a lot of use cases that are starting to be built up. We need to understand those use cases and be able to draw inferences from them to more effectively design programs using AI in the future. One way that this has been used is in AI marketing, which would be leveraging AI tools and methods such as large language models, to basically develop insights around I'll use the term consumer, but you could also  think of those as people, as beneficiaries, if we're in the public health world, trying to help people change their behaviors for good and also to personalize the offerings that we're making. So these kinds of approaches, yes, they're being used very much in the commercial world, but they can also be applied to promoting pro social behaviors, as I'll try to argue and illustrate here in a second. In a recent paper, with colleagues Marco bartis and Jeff French, we identified six key benefits of applying AI as part of behavioral change programs, and those are the ability to develop more personalized and tailored supports to increase scale and reach, to increase engagement in programs, so getting making programs interesting engaging, having people stay stay with them longer, by maintaining interest in a topic, also spotting trends and being able to respond rapidly to, for example, emerging public health threats like the next pandemic, would be a good example. And also building communities of interest in providing support. So one example of this that we talked about in the paper was the idea that generative AI can be used to address issues, for example, like competition with unhealthy behaviors, by examining large data sets, identifying user patterns where people are potentially engaging in unhealthy behaviors, And then developing based on those large data sets, better offers of exchanges that are more beneficial and thereby out compete the competition. So there's a concept that I've used and been applying in my research for a while now, which is the idea of digital segmentation. So one way of thinking about this is like the the technology in social media for retargeting, or it's sometimes called remarketing, and basically we can use this to segment and target content in online offerings to customized audiences, to very precisely defined audiences based On available data. And AI basically makes us enables us to very precisely targeted segment and to recruit participants in the studies based on those precise targets and segments. So intervention studies can use retargeting to basically redirect content very specifically to customized audiences and also to titrate how much of that content is delivered. So you can basically design naturalistic, randomized, controlled trials or or quasi experiments, and look at the effects of delivering more versus less content, different types of content, potentially comparative effectiveness sorts of studies. And all of this can be done through AI enabled Social Media Research. There's a lot of other ways in which we can use AI for digital behavior change research, but I'm going to talk about this one specific area today for in the interest of time. One example of a platform that allows you to do this is the virtual lab platform that I have worked with for a number of years now. And be happy to talk to you about more about that in the Q and A segment, just to put a little more mean on the bone here. Basically
think of those as people, as beneficiaries, if we're in the public health world, trying to help people change their behaviors for good and also to personalize the offerings that we're making. So these kinds of approaches, yes, they're being used very much in the commercial world, but they can also be applied to promoting pro social behaviors, as I'll try to argue and illustrate here in a second. In a recent paper, with colleagues Marco bartis and Jeff French, we identified six key benefits of applying AI as part of behavioral change programs, and those are the ability to develop more personalized and tailored supports to increase scale and reach, to increase engagement in programs, so getting making programs interesting engaging, having people stay stay with them longer, by maintaining interest in a topic, also spotting trends and being able to respond rapidly to, for example, emerging public health threats like the next pandemic, would be a good example. And also building communities of interest in providing support. So one example of this that we talked about in the paper was the idea that generative AI can be used to address issues, for example, like competition with unhealthy behaviors, by examining large data sets, identifying user patterns where people are potentially engaging in unhealthy behaviors, And then developing based on those large data sets, better offers of exchanges that are more beneficial and thereby out compete the competition. So there's a concept that I've used and been applying in my research for a while now, which is the idea of digital segmentation. So one way of thinking about this is like the the technology in social media for retargeting, or it's sometimes called remarketing, and basically we can use this to segment and target content in online offerings to customized audiences, to very precisely defined audiences based On available data. And AI basically makes us enables us to very precisely targeted segment and to recruit participants in the studies based on those precise targets and segments. So intervention studies can use retargeting to basically redirect content very specifically to customized audiences and also to titrate how much of that content is delivered. So you can basically design naturalistic, randomized, controlled trials or or quasi experiments, and look at the effects of delivering more versus less content, different types of content, potentially comparative effectiveness sorts of studies. And all of this can be done through AI enabled Social Media Research. There's a lot of other ways in which we can use AI for digital behavior change research, but I'm going to talk about this one specific area today for in the interest of time. One example of a platform that allows you to do this is the virtual lab platform that I have worked with for a number of years now. And be happy to talk to you about more about that in the Q and A segment, just to put a little more mean on the bone here. Basically  one thing you can do is to take like the meta platforms, for example, Instagram, Facebook and so forth. And these have been used for years now by businesses to target content based on demographics, interest, your online behavior, where you live and so forth, and so you can basically create custom audience lists based on combinations of user data. So for example, like demographics plus online activity, you develop a very precise segment, and you can market content that's more relevant to that segment. That information can be used to direct content to users. And behavioral interventions can use exactly the same approach as I'll show you in a second. So the basic idea of retargeting, for example, if a user maybe is interested in getting an online data degree, or they want to go to University of Maryland or GW, or something like that, and get an online degree, well, okay, you're going to get this content that's relevant to that area of interest, and maybe to who you know the AI thinks you are in this case, so an example of an ad that you might get there. So that's basically the idea of retargeting. So we've been using this technology to do online research. I've done a number of studies using this in the past few years on topics like vaccination, maternal and child health, obesity prevention, and in particular, nicotine use prevention, smoking and vaping prevention. So I'll talk about that briefly. Just to illustrate this idea, we used retargeting to identify social media users who were young adults, 18 to 24 year olds living in the USA, and we recruited them into an intervention using paid advertising on social media, on the meta platforms, and we designed a randomized control trial to examine vaping and smoking outcomes, and then we did a 30 and 60 day follow ups. We rapidly recruited over 1800 participants, and we were able to randomize them to different levels of exposure. So basically, once they're recruited into the study, we can direct content to those individuals based on what study. So these were for campaign themed anti vaping ads. I'll show you an example in a second. And we basically were attempting to apply a dose response curve of exposures and then examining the effects of exposure levels on different outcomes related to vaping over a 60 day period.
one thing you can do is to take like the meta platforms, for example, Instagram, Facebook and so forth. And these have been used for years now by businesses to target content based on demographics, interest, your online behavior, where you live and so forth, and so you can basically create custom audience lists based on combinations of user data. So for example, like demographics plus online activity, you develop a very precise segment, and you can market content that's more relevant to that segment. That information can be used to direct content to users. And behavioral interventions can use exactly the same approach as I'll show you in a second. So the basic idea of retargeting, for example, if a user maybe is interested in getting an online data degree, or they want to go to University of Maryland or GW, or something like that, and get an online degree, well, okay, you're going to get this content that's relevant to that area of interest, and maybe to who you know the AI thinks you are in this case, so an example of an ad that you might get there. So that's basically the idea of retargeting. So we've been using this technology to do online research. I've done a number of studies using this in the past few years on topics like vaccination, maternal and child health, obesity prevention, and in particular, nicotine use prevention, smoking and vaping prevention. So I'll talk about that briefly. Just to illustrate this idea, we used retargeting to identify social media users who were young adults, 18 to 24 year olds living in the USA, and we recruited them into an intervention using paid advertising on social media, on the meta platforms, and we designed a randomized control trial to examine vaping and smoking outcomes, and then we did a 30 and 60 day follow ups. We rapidly recruited over 1800 participants, and we were able to randomize them to different levels of exposure. So basically, once they're recruited into the study, we can direct content to those individuals based on what study. So these were for campaign themed anti vaping ads. I'll show you an example in a second. And we basically were attempting to apply a dose response curve of exposures and then examining the effects of exposure levels on different outcomes related to vaping over a 60 day period. 
 All of this is delivered by Chatbot. So it's an AI enabled study, and so we were using social media to identify the audience segments, and you see the basic study design here, how we recruited and randomized them so people weren't eligible, and then the AI based chat bot was used to recruit people, and then we screened them into the study using chats, Using the Facebook Messenger app to confirm eligibility. These are just some examples of recruitment ads. We kind of got a little bit more sophisticated as we went through and developed slightly
All of this is delivered by Chatbot. So it's an AI enabled study, and so we were using social media to identify the audience segments, and you see the basic study design here, how we recruited and randomized them so people weren't eligible, and then the AI based chat bot was used to recruit people, and then we screened them into the study using chats, Using the Facebook Messenger app to confirm eligibility. These are just some examples of recruitment ads. We kind of got a little bit more sophisticated as we went through and developed slightly
+3
you very much. Let me share my screen. Right place here. Give me a second. Hey, hopefully you can see that. Yep, all right, great. Well, thank you all very much. I am going to present on my work on social and behavioral change using AI. And let me just start off by talking broadly about the work that we do here at the bright Institute at GW. So I view using the use of AI for social and behavioral change as falling within the broader field of digital health interventions, or DHS, as they've been defined in the literature. And what I mean by that are basically any kind of program intervention campaign aimed at changing specific behaviors in a population, using digital platforms for the delivery of that intervention and also research to evaluate the effectiveness of those kinds of programs. But a big question that we talked about in a paper a couple of years ago is, how effective are these programs, and under what conditions do they work? They don't necessarily work under all conditions, and we need to understand that context much better than we do now. So AI can definitely be used for social good. There's a lot of discussion out in the media and many areas of literature that talk about all the negatives of AI, but it's definitely the case that AI can be a major force for social good. The McKenzie Institute, just as an example, tried to kind of categorize this idea a few years ago, and they identified these 10 domains of areas in which AI has been shown to be affected to at least a certain extent, in promoting pro social causes and goods. So economic empowerment, education, infrastructure, public and social sector factors, combating false news or polarization, potentially, although, of course, AI can also create those problems. So it's clear that AI can be used for social good, and we have a lot of use cases that are starting to be built up. We need to understand those use cases and be able to draw inferences from them to more effectively design programs using AI in the future. One way that this has been used is in AI marketing, which would be leveraging AI tools and methods such as large language models, to basically develop insights around I'll use the term consumer, but you could also 
+1
think of those as people, as beneficiaries, if we're in the public health world, trying to help people change their behaviors for good and also to personalize the offerings that we're making. So these kinds of approaches, yes, they're being used very much in the commercial world, but they can also be applied to promoting pro social behaviors, as I'll try to argue and illustrate here in a second. In a recent paper, with colleagues Marco bartis and Jeff French, we identified six key benefits of applying AI as part of behavioral change programs, and those are the ability to develop more personalized and tailored supports to increase scale and reach, to increase engagement in programs, so getting making programs interesting engaging, having people stay stay with them longer, by maintaining interest in a topic, also spotting trends and being able to respond rapidly to, for example, emerging public health threats like the next pandemic, would be a good example. And also building communities of interest in providing support. So one example of this that we talked about in the paper was the idea that generative AI can be used to address issues, for example, like competition with unhealthy behaviors, by examining large data sets, identifying user patterns where people are potentially engaging in unhealthy behaviors, And then developing based on those large data sets, better offers of exchanges that are more beneficial and thereby out compete the competition. So there's a concept that I've used and been applying in my research for a while now, which is the idea of digital segmentation. So one way of thinking about this is like the the technology in social media for retargeting, or it's sometimes called remarketing, and basically we can use this to segment and target content in online offerings to customized audiences, to very precisely defined audiences based On available data. And AI basically makes us enables us to very precisely targeted segment and to recruit participants in the studies based on those precise targets and segments. So intervention studies can use retargeting to basically redirect content very specifically to customized audiences and also to titrate how much of that content is delivered. So you can basically design naturalistic, randomized, controlled trials or or quasi experiments, and look at the effects of delivering more versus less content, different types of content, potentially comparative effectiveness sorts of studies. And all of this can be done through AI enabled Social Media Research. There's a lot of other ways in which we can use AI for digital behavior change research, but I'm going to talk about this one specific area today for in the interest of time. One example of a platform that allows you to do this is the virtual lab platform that I have worked with for a number of years now. And be happy to talk to you about more about that in the Q and A segment, just to put a little more mean on the bone here. Basically +1
one thing you can do is to take like the meta platforms, for example, Instagram, Facebook and so forth. And these have been used for years now by businesses to target content based on demographics, interest, your online behavior, where you live and so forth, and so you can basically create custom audience lists based on combinations of user data. So for example, like demographics plus online activity, you develop a very precise segment, and you can market content that's more relevant to that segment. That information can be used to direct content to users. And behavioral interventions can use exactly the same approach as I'll show you in a second. So the basic idea of retargeting, for example, if a user maybe is interested in getting an online data degree, or they want to go to University of Maryland or GW, or something like that, and get an online degree, well, okay, you're going to get this content that's relevant to that area of interest, and maybe to who you know the AI thinks you are in this case, so an example of an ad that you might get there. So that's basically the idea of retargeting. So we've been using this technology to do online research. I've done a number of studies using this in the past few years on topics like vaccination, maternal and child health, obesity prevention, and in particular, nicotine use prevention, smoking and vaping prevention. So I'll talk about that briefly. Just to illustrate this idea, we used retargeting to identify social media users who were young adults, 18 to 24 year olds living in the USA, and we recruited them into an intervention using paid advertising on social media, on the meta platforms, and we designed a randomized control trial to examine vaping and smoking outcomes, and then we did a 30 and 60 day follow ups. We rapidly recruited over 1800 participants, and we were able to randomize them to different levels of exposure. So basically, once they're recruited into the study, we can direct content to those individuals based on what study. So these were for campaign themed anti vaping ads. I'll show you an example in a second. And we basically were attempting to apply a dose response curve of exposures and then examining the effects of exposure levels on different outcomes related to vaping over a 60 day period. +2
All of this is delivered by Chatbot. So it's an AI enabled study, and so we were using social media to identify the audience segments, and you see the basic study design here, how we recruited and randomized them so people weren't eligible, and then the AI based chat bot was used to recruit people, and then we screened them into the study using chats, Using the Facebook Messenger app to confirm eligibility. These are just some examples of recruitment ads. We kind of got a little bit more sophisticated as we went through and developed slightly Speaker 1
this 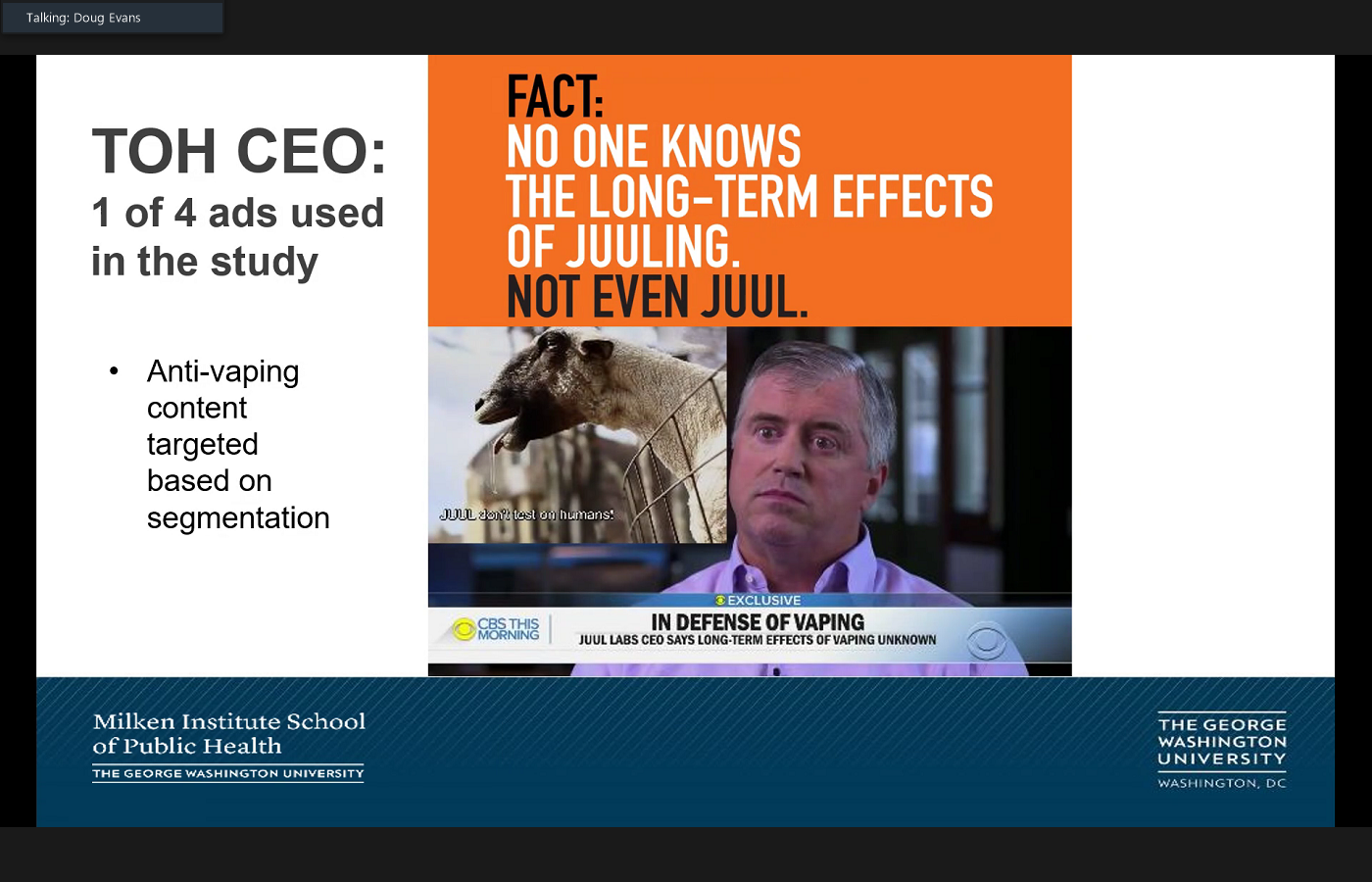
 kind of static, generic, Amazon, get some Amazon money, add to something slightly here works anyway, and we use social media segmentation by to advertise to these young adults. And the chat bot, as I said, was used for recruitment, and then we recruited into the research using that segmentation. This is one of the ads that the videos that was used anti vaping content based on that segmentation. And this is actually an excerpt from CVS this morning where the CEO of Juul is essentially admitting that no one really knows the long term effects of juuling. Not even Juul whatever, a damning admission, I would say, pretty hard hitting piece of content. And here's another example of a branded anti vaping ad from the truth initiative, our partners at truth initiative, that was used in the study.
kind of static, generic, Amazon, get some Amazon money, add to something slightly here works anyway, and we use social media segmentation by to advertise to these young adults. And the chat bot, as I said, was used for recruitment, and then we recruited into the research using that segmentation. This is one of the ads that the videos that was used anti vaping content based on that segmentation. And this is actually an excerpt from CVS this morning where the CEO of Juul is essentially admitting that no one really knows the long term effects of juuling. Not even Juul whatever, a damning admission, I would say, pretty hard hitting piece of content. And here's another example of a branded anti vaping ad from the truth initiative, our partners at truth initiative, that was used in the study.
+2
kind of static, generic, Amazon, get some Amazon money, add to something slightly here works anyway, and we use social media segmentation by to advertise to these young adults. And the chat bot, as I said, was used for recruitment, and then we recruited into the research using that segmentation. This is one of the ads that the videos that was used anti vaping content based on that segmentation. And this is actually an excerpt from CVS this morning where the CEO of Juul is essentially admitting that no one really knows the long term effects of juuling. Not even Juul whatever, a damning admission, I would say, pretty hard hitting piece of content. And here's another example of a branded anti vaping ad from the truth initiative, our partners at truth initiative, that was used in the study. Speaker 2
I feel like you don't want me to be happy. You only ever wanted my money. You're just like your mother.
Unknown Speaker
Oh, depression's
Speaker 1
thick,  again, trying to appeal to humor and and also, clearly, we could use AI and the results of the research that we're doing to create even more entertaining, more engaging ads for the audience. When we ran this RCT over 60 days, we found reduced vape use intentions at follow up among treatment current users compared to control. So the intervention was effective among current vapors, and we also increased anti vape industry beliefs. So basically, the belief that the vaping industry is trying to manipulate you, trying to cause harm to you among current vapors, compared to control. So we demonstrated evidence of effectiveness in this trial, and that's been published in the Journal of Medical internet research. As I wrap up, there are a lot of future research and challenges in this field. How do we expand and improve the use of AI? There are a lot of AI for behavior change challenges. I think, for example, biased inputs, the potential to reinforce inequalities. We're not really engaging in an interpersonal interaction. Is that going to be lost if we really emphasize these kinds of interventions over interpersonal interventions? What's the balance? What's the right balance there? And also these biases may lead to unrealistic goals or program expectations. We need to try to combat those and use the AI, the data that we're gathering through our studies, using AI to actually improve the quality of those studies based on on the AI. So future research really needs to keep up with changing technologies and also figure out how to translate our research findings into public health impact. And I'll be happy to answer questions later on, and let me stop
again, trying to appeal to humor and and also, clearly, we could use AI and the results of the research that we're doing to create even more entertaining, more engaging ads for the audience. When we ran this RCT over 60 days, we found reduced vape use intentions at follow up among treatment current users compared to control. So the intervention was effective among current vapors, and we also increased anti vape industry beliefs. So basically, the belief that the vaping industry is trying to manipulate you, trying to cause harm to you among current vapors, compared to control. So we demonstrated evidence of effectiveness in this trial, and that's been published in the Journal of Medical internet research. As I wrap up, there are a lot of future research and challenges in this field. How do we expand and improve the use of AI? There are a lot of AI for behavior change challenges. I think, for example, biased inputs, the potential to reinforce inequalities. We're not really engaging in an interpersonal interaction. Is that going to be lost if we really emphasize these kinds of interventions over interpersonal interventions? What's the balance? What's the right balance there? And also these biases may lead to unrealistic goals or program expectations. We need to try to combat those and use the AI, the data that we're gathering through our studies, using AI to actually improve the quality of those studies based on on the AI. So future research really needs to keep up with changing technologies and also figure out how to translate our research findings into public health impact. And I'll be happy to answer questions later on, and let me stop
+1
again, trying to appeal to humor and and also, clearly, we could use AI and the results of the research that we're doing to create even more entertaining, more engaging ads for the audience. When we ran this RCT over 60 days, we found reduced vape use intentions at follow up among treatment current users compared to control. So the intervention was effective among current vapors, and we also increased anti vape industry beliefs. So basically, the belief that the vaping industry is trying to manipulate you, trying to cause harm to you among current vapors, compared to control. So we demonstrated evidence of effectiveness in this trial, and that's been published in the Journal of Medical internet research. As I wrap up, there are a lot of future research and challenges in this field. How do we expand and improve the use of AI? There are a lot of AI for behavior change challenges. I think, for example, biased inputs, the potential to reinforce inequalities. We're not really engaging in an interpersonal interaction. Is that going to be lost if we really emphasize these kinds of interventions over interpersonal interventions? What's the balance? What's the right balance there? And also these biases may lead to unrealistic goals or program expectations. We need to try to combat those and use the AI, the data that we're gathering through our studies, using AI to actually improve the quality of those studies based on on the AI. So future research really needs to keep up with changing technologies and also figure out how to translate our research findings into public health impact. And I'll be happy to answer questions later on, and let me stop Unknown Speaker
hearing thank you so much. Doug, that was great, and now we'll turn it over to our third presenter, Catarina bots. You
Unknown Speaker
so  I don't know if you can see my screen. Yeah. So hi everyone. Thank you very much for inviting me. Thank you for the introduction earlier, Lorien abroms, as Lorien said, my name is Katerina botsiou, who and I work in the communications department in who headquarters here in Geneva. It's a pleasure to be here today and to be able to share with you the work that we as who have been doing in the digital field. Today. I'm here to talk to you about our AI enabled virtual human that we launched recently, Sarah. But I would like to start with giving you an overview of all our chat bots and Sarah's predecessor, Florence, because Sarah is part of the of who's digital health communications ecosystem. But let's start with the basics. What does who do with digital technologies? So as you know, who is the UN specialized agency for health we work on health guidelines, standards, policies and programs around the world with our 194 member states, we work on all health topics, and our work touches on everyone's lives, from keeping people healthy and well, to ensuring that health systems are functioning well well when they do fall sick, and, of course, protecting people from health emergencies. In terms of digital who is interested in new technologies as a way to to expand access to health and health information, as with any other area of health, we are led by evidence. And whilst we're very much interested in innovative ways to reach people through digital, we must always make sure that our work is evidence based. We're also interested in the broader environment for digital such as security, privacy, data, ownership, confidentiality and, of course, any ethical concerns. So during covid and with the healthcare systems around the world overwhelmed millions of people during that time, relied on digital to either for advice, for doing remote consultations with doctors to check symptoms and more. So we immediately identified the need to to find alternative ways to reach out to people with health information around the coronavirus. So during that time, there was something else that was circulating on the digital sphere, and that was the spread of misinformation. We all remember some, even anecdotal ones, like, if you eat garlic, you can cure yourself from covid, and how fast all these spread. So this is dangerous and an example on how false information can spread and its impact and health inequalities that can become worse because of it. So in order to harness the benefits of digital and to effectively combat misinformation, who has looked at the use of chatbots, the idea was that we need to reach people where they are. So we thought, Where do we spend most of our times every day? On our phones? The average person has something like 40 apps installed on their phone, but on a daily basis, we use no more than four or five. So what we did did is we partnered with messaging apps such as Facebook, Viber, WhatsApp and free basics to get up to date covid information out to as many people as possible. Now, unlike human experts, these chatbots can talk to millions of people in their preferred language on their preferred platform, anywhere at any time. And the WHO chatbots are currently available in 26 languages and have reached over 20 million users. People can interact with them to get information on covid prevention measures, how to stop the spread, and over time, we added content on stress management, women's health and tobacco cessation. On tobacco cessation, specifically, we worked on a 42 day challenge that is still active on WhatsApp, Viper and Facebook Messenger, and we have also worked with partners to to work on building the first digital AI health worker that can help people who quit tobacco, old Florence. So as I said, Florence is who's first ever digital health worker. She She essentially is an autonomously animated digital person that was launched on the WHO website in july 2020, and was created in partnership between who soul machines, Google and Amazon Web Services. During this first iteration, she was using a predefined corpus, and could speak to users about covid 19, covid 19 vaccines, Mythbusters around covid, tobacco cessation and its link to covid. She could also help users make a quitting plan, and also refer them to toll free quit lines and apps that could help them on their quitting journey. A bit later on, and as we were moving away from covid, Florence 2.0 was launched, and she was launched as a global ambassador on NCDs, non communicable diseases. So in addition to the topics that she could already speak about, she was expanded to cover epithelial topics on NCDs, such as physical activity, healthy eating and mental health, but mostly in the sense of stress management. I would now like to introduce you to Sarah so recently, and more specifically, in april 2024 who relaunched Florence, as you can see in the picture, the way she looks has been changed, but this was actually changed during the transition between the Florence 1.0 to 2.0 version. But yeah, now she looks different and different, and she has also been renamed to Sarah. Sarah is an acronym for a smart AI resource assistant for health. Sara is a prototype. She's a prototype digital health promoter, and the big difference to her predecessor is that she's now using generative AI to help people live healthier lives. She has been trained with information from the World Health Organization and trusted partners, and although she can speak about a variety of topic, she specializes in tobacco and E cigarettes, mental health, nutrition, physical activity, cancer and diabetes. Users can speak to Sarah by video or text on any device around the clock. She's currently available in eight languages, the six Yuan languages, so English, French, Spanish, Arabic, Russian and Chinese, plus Hindi and Portuguese. But in theory, she has the potential to speak any language that is supported by OpenAI. Sarah has enhanced conversational skills, can show empathy by mirroring people's facial expressions, and harnesses the power of AI to speak in a more personalized and engaged, engaging way. And I think it's important to stress that all conversations with Sarah are anonymous and non identifiable, and Sarah illustrates the potential of artificial intelligence to deliver health information to anyone with an Internet connection, and is by no means to be considered a medical a medical tool, as I said,
I don't know if you can see my screen. Yeah. So hi everyone. Thank you very much for inviting me. Thank you for the introduction earlier, Lorien abroms, as Lorien said, my name is Katerina botsiou, who and I work in the communications department in who headquarters here in Geneva. It's a pleasure to be here today and to be able to share with you the work that we as who have been doing in the digital field. Today. I'm here to talk to you about our AI enabled virtual human that we launched recently, Sarah. But I would like to start with giving you an overview of all our chat bots and Sarah's predecessor, Florence, because Sarah is part of the of who's digital health communications ecosystem. But let's start with the basics. What does who do with digital technologies? So as you know, who is the UN specialized agency for health we work on health guidelines, standards, policies and programs around the world with our 194 member states, we work on all health topics, and our work touches on everyone's lives, from keeping people healthy and well, to ensuring that health systems are functioning well well when they do fall sick, and, of course, protecting people from health emergencies. In terms of digital who is interested in new technologies as a way to to expand access to health and health information, as with any other area of health, we are led by evidence. And whilst we're very much interested in innovative ways to reach people through digital, we must always make sure that our work is evidence based. We're also interested in the broader environment for digital such as security, privacy, data, ownership, confidentiality and, of course, any ethical concerns. So during covid and with the healthcare systems around the world overwhelmed millions of people during that time, relied on digital to either for advice, for doing remote consultations with doctors to check symptoms and more. So we immediately identified the need to to find alternative ways to reach out to people with health information around the coronavirus. So during that time, there was something else that was circulating on the digital sphere, and that was the spread of misinformation. We all remember some, even anecdotal ones, like, if you eat garlic, you can cure yourself from covid, and how fast all these spread. So this is dangerous and an example on how false information can spread and its impact and health inequalities that can become worse because of it. So in order to harness the benefits of digital and to effectively combat misinformation, who has looked at the use of chatbots, the idea was that we need to reach people where they are. So we thought, Where do we spend most of our times every day? On our phones? The average person has something like 40 apps installed on their phone, but on a daily basis, we use no more than four or five. So what we did did is we partnered with messaging apps such as Facebook, Viber, WhatsApp and free basics to get up to date covid information out to as many people as possible. Now, unlike human experts, these chatbots can talk to millions of people in their preferred language on their preferred platform, anywhere at any time. And the WHO chatbots are currently available in 26 languages and have reached over 20 million users. People can interact with them to get information on covid prevention measures, how to stop the spread, and over time, we added content on stress management, women's health and tobacco cessation. On tobacco cessation, specifically, we worked on a 42 day challenge that is still active on WhatsApp, Viper and Facebook Messenger, and we have also worked with partners to to work on building the first digital AI health worker that can help people who quit tobacco, old Florence. So as I said, Florence is who's first ever digital health worker. She She essentially is an autonomously animated digital person that was launched on the WHO website in july 2020, and was created in partnership between who soul machines, Google and Amazon Web Services. During this first iteration, she was using a predefined corpus, and could speak to users about covid 19, covid 19 vaccines, Mythbusters around covid, tobacco cessation and its link to covid. She could also help users make a quitting plan, and also refer them to toll free quit lines and apps that could help them on their quitting journey. A bit later on, and as we were moving away from covid, Florence 2.0 was launched, and she was launched as a global ambassador on NCDs, non communicable diseases. So in addition to the topics that she could already speak about, she was expanded to cover epithelial topics on NCDs, such as physical activity, healthy eating and mental health, but mostly in the sense of stress management. I would now like to introduce you to Sarah so recently, and more specifically, in april 2024 who relaunched Florence, as you can see in the picture, the way she looks has been changed, but this was actually changed during the transition between the Florence 1.0 to 2.0 version. But yeah, now she looks different and different, and she has also been renamed to Sarah. Sarah is an acronym for a smart AI resource assistant for health. Sara is a prototype. She's a prototype digital health promoter, and the big difference to her predecessor is that she's now using generative AI to help people live healthier lives. She has been trained with information from the World Health Organization and trusted partners, and although she can speak about a variety of topic, she specializes in tobacco and E cigarettes, mental health, nutrition, physical activity, cancer and diabetes. Users can speak to Sarah by video or text on any device around the clock. She's currently available in eight languages, the six Yuan languages, so English, French, Spanish, Arabic, Russian and Chinese, plus Hindi and Portuguese. But in theory, she has the potential to speak any language that is supported by OpenAI. Sarah has enhanced conversational skills, can show empathy by mirroring people's facial expressions, and harnesses the power of AI to speak in a more personalized and engaged, engaging way. And I think it's important to stress that all conversations with Sarah are anonymous and non identifiable, and Sarah illustrates the potential of artificial intelligence to deliver health information to anyone with an Internet connection, and is by no means to be considered a medical a medical tool, as I said, 
 She's powered by generative AI, and we have put in place guardrails in order to make SATA source reliable evidence backed information, we do take we have taken a user centric approach with SATA, and we do take user feedback very seriously, we have put a survey in Place. This survey can be accessed either on the WHO landing page for Sarah or while in conversation with her. And in this slide, I would like to show you some of the user quotes that we have received in the first two months since Sarah's launch. So Sarah has been really helpful. I'm happy today as I found Sara as my supportive hand. I'll talk to Sarah whenever I need to talk to her. Sarah is very helpful. At times you don't want to share your secrets with anyone, yet it is very depressing, and sharing would help. So Sara is the right person to share with, since she doesn't know me and will not judge me and such a great way to increase access to mental health services. But I think I will stop here and let Sarah speak for herself.
She's powered by generative AI, and we have put in place guardrails in order to make SATA source reliable evidence backed information, we do take we have taken a user centric approach with SATA, and we do take user feedback very seriously, we have put a survey in Place. This survey can be accessed either on the WHO landing page for Sarah or while in conversation with her. And in this slide, I would like to show you some of the user quotes that we have received in the first two months since Sarah's launch. So Sarah has been really helpful. I'm happy today as I found Sara as my supportive hand. I'll talk to Sarah whenever I need to talk to her. Sarah is very helpful. At times you don't want to share your secrets with anyone, yet it is very depressing, and sharing would help. So Sara is the right person to share with, since she doesn't know me and will not judge me and such a great way to increase access to mental health services. But I think I will stop here and let Sarah speak for herself.
+1
I don't know if you can see my screen. Yeah. So hi everyone. Thank you very much for inviting me. Thank you for the introduction earlier, Lorien abroms, as Lorien said, my name is Katerina botsiou, who and I work in the communications department in who headquarters here in Geneva. It's a pleasure to be here today and to be able to share with you the work that we as who have been doing in the digital field. Today. I'm here to talk to you about our AI enabled virtual human that we launched recently, Sarah. But I would like to start with giving you an overview of all our chat bots and Sarah's predecessor, Florence, because Sarah is part of the of who's digital health communications ecosystem. But let's start with the basics. What does who do with digital technologies? So as you know, who is the UN specialized agency for health we work on health guidelines, standards, policies and programs around the world with our 194 member states, we work on all health topics, and our work touches on everyone's lives, from keeping people healthy and well, to ensuring that health systems are functioning well well when they do fall sick, and, of course, protecting people from health emergencies. In terms of digital who is interested in new technologies as a way to to expand access to health and health information, as with any other area of health, we are led by evidence. And whilst we're very much interested in innovative ways to reach people through digital, we must always make sure that our work is evidence based. We're also interested in the broader environment for digital such as security, privacy, data, ownership, confidentiality and, of course, any ethical concerns. So during covid and with the healthcare systems around the world overwhelmed millions of people during that time, relied on digital to either for advice, for doing remote consultations with doctors to check symptoms and more. So we immediately identified the need to to find alternative ways to reach out to people with health information around the coronavirus. So during that time, there was something else that was circulating on the digital sphere, and that was the spread of misinformation. We all remember some, even anecdotal ones, like, if you eat garlic, you can cure yourself from covid, and how fast all these spread. So this is dangerous and an example on how false information can spread and its impact and health inequalities that can become worse because of it. So in order to harness the benefits of digital and to effectively combat misinformation, who has looked at the use of chatbots, the idea was that we need to reach people where they are. So we thought, Where do we spend most of our times every day? On our phones? The average person has something like 40 apps installed on their phone, but on a daily basis, we use no more than four or five. So what we did did is we partnered with messaging apps such as Facebook, Viber, WhatsApp and free basics to get up to date covid information out to as many people as possible. Now, unlike human experts, these chatbots can talk to millions of people in their preferred language on their preferred platform, anywhere at any time. And the WHO chatbots are currently available in 26 languages and have reached over 20 million users. People can interact with them to get information on covid prevention measures, how to stop the spread, and over time, we added content on stress management, women's health and tobacco cessation. On tobacco cessation, specifically, we worked on a 42 day challenge that is still active on WhatsApp, Viper and Facebook Messenger, and we have also worked with partners to to work on building the first digital AI health worker that can help people who quit tobacco, old Florence. So as I said, Florence is who's first ever digital health worker. She She essentially is an autonomously animated digital person that was launched on the WHO website in july 2020, and was created in partnership between who soul machines, Google and Amazon Web Services. During this first iteration, she was using a predefined corpus, and could speak to users about covid 19, covid 19 vaccines, Mythbusters around covid, tobacco cessation and its link to covid. She could also help users make a quitting plan, and also refer them to toll free quit lines and apps that could help them on their quitting journey. A bit later on, and as we were moving away from covid, Florence 2.0 was launched, and she was launched as a global ambassador on NCDs, non communicable diseases. So in addition to the topics that she could already speak about, she was expanded to cover epithelial topics on NCDs, such as physical activity, healthy eating and mental health, but mostly in the sense of stress management. I would now like to introduce you to Sarah so recently, and more specifically, in april 2024 who relaunched Florence, as you can see in the picture, the way she looks has been changed, but this was actually changed during the transition between the Florence 1.0 to 2.0 version. But yeah, now she looks different and different, and she has also been renamed to Sarah. Sarah is an acronym for a smart AI resource assistant for health. Sara is a prototype. She's a prototype digital health promoter, and the big difference to her predecessor is that she's now using generative AI to help people live healthier lives. She has been trained with information from the World Health Organization and trusted partners, and although she can speak about a variety of topic, she specializes in tobacco and E cigarettes, mental health, nutrition, physical activity, cancer and diabetes. Users can speak to Sarah by video or text on any device around the clock. She's currently available in eight languages, the six Yuan languages, so English, French, Spanish, Arabic, Russian and Chinese, plus Hindi and Portuguese. But in theory, she has the potential to speak any language that is supported by OpenAI. Sarah has enhanced conversational skills, can show empathy by mirroring people's facial expressions, and harnesses the power of AI to speak in a more personalized and engaged, engaging way. And I think it's important to stress that all conversations with Sarah are anonymous and non identifiable, and Sarah illustrates the potential of artificial intelligence to deliver health information to anyone with an Internet connection, and is by no means to be considered a medical a medical tool, as I said, +5
She's powered by generative AI, and we have put in place guardrails in order to make SATA source reliable evidence backed information, we do take we have taken a user centric approach with SATA, and we do take user feedback very seriously, we have put a survey in Place. This survey can be accessed either on the WHO landing page for Sarah or while in conversation with her. And in this slide, I would like to show you some of the user quotes that we have received in the first two months since Sarah's launch. So Sarah has been really helpful. I'm happy today as I found Sara as my supportive hand. I'll talk to Sarah whenever I need to talk to her. Sarah is very helpful. At times you don't want to share your secrets with anyone, yet it is very depressing, and sharing would help. So Sara is the right person to share with, since she doesn't know me and will not judge me and such a great way to increase access to mental health services. But I think I will stop here and let Sarah speak for herself. 

