Loading...
DWIHN — Finance Committee, 6/4/2025
Speaker 1
Oh, Lord, let's wear my chair so Hot I feel like I'm Sitting you.
Speaker 1
Good afternoon everyone? Good afternoon. Recording in progress.
Unknown Speaker
Who else was that good afternoon? Everyone?
Speaker 1
I apologize for the delay. We are getting ready to start the Finance Committee meeting at 1:06pm you
Unknown Speaker
I would like to call the meeting to order.
Unknown Speaker
Can I get a roll call please?
Speaker 2
Yes. Madam Chair, Dr tag, thank you, Mr. McNamara, here. Thank you. Mr. Parker, thank you. Ms, brown present, thank you. Ms, Garza de Walsh, thank you.
Unknown Speaker
Ms, Ruth present, thank you.
Speaker 2
Are there any committee members or board members joining the Finance Committee meeting via zoom.
Unknown Speaker
Hearing none. Madam Chair, you do have a quorum?
Speaker 1
Thank you. Do we have any committee member remarks?
Speaker 2
Madam Chair, I'm sorry. Commissioner Kinloch is joining us today.
Speaker 1
Thank you. I thought you called his name. No, okay
Unknown Speaker
again. Do we have any committee member remarks?
Speaker 1
Can I get an approval of the agenda? Please? So move Madam Chair. Properly moved and supported All in favor, aye, anyone opposed, any discussion,
Unknown Speaker
follow up items.
Speaker 1
Provide information on the Mental Health Act fund. We deferred program Compliance Committee. I uh, to ask them if there were any Sud programs or programs that were impacted by the loss of the COVID grants. And then we were also asked to we asked that we have an analysis of the number of contracts over the last two years that have gone to the board between 50 and $100,000
Speaker 3
yes, 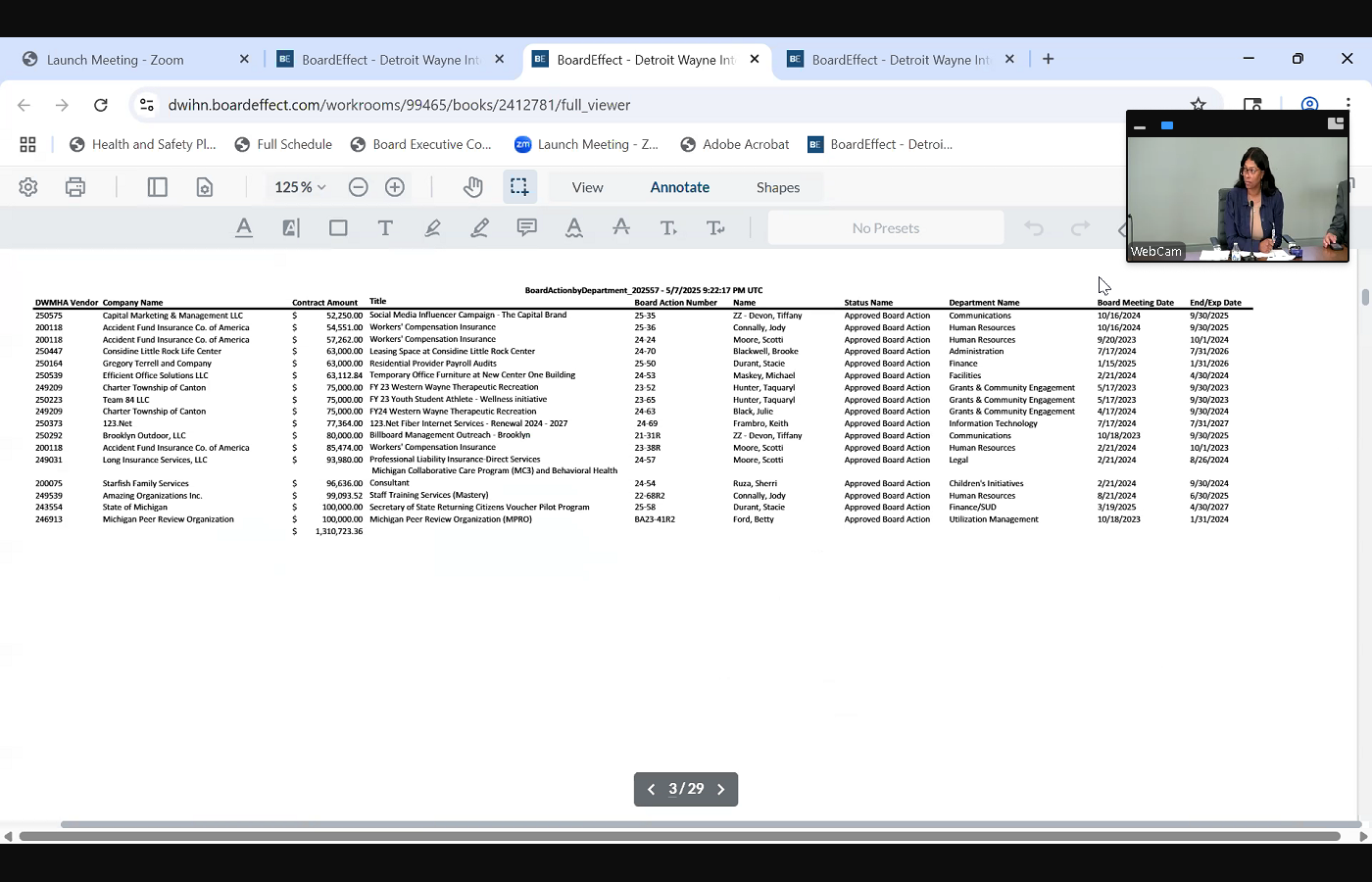
 ma'am, through the chair. The first item was, if, just, if you recall from the last meeting, this body asked me for an analysis of how much, which grant, which COVID funds, were impacted by the the federal cease of COVID grants, and I presented that information to you all, and then you are deferred. It's a Compliance Committee to, I'm sorry not to PCC program compliance in order to determine the impact if any of the I of the the march 31 deadline on those grants. So that's and then the In addition, at the last meeting, there was a presentation of amendment to the procurement policy, and it was deferred or requested. It was passed with, you know, to go to policy. Policy got canceled, so I brought the list to finance. It'll also go to policy if you guys wanted as well. But because policy got canceled, I did bring that list of any grant, any contracts, between 50 and 100,000 because one of the request of this body was approve a change that board actions under 100,000 or but board actions over 100,000 come to to the board opposed to 50,000 so that document is included in This packet. You guys, I think, initially asked for one year, and I said I would provide two years. So there is a document and in the packet that details those board actions between 50 and 100,000
ma'am, through the chair. The first item was, if, just, if you recall from the last meeting, this body asked me for an analysis of how much, which grant, which COVID funds, were impacted by the the federal cease of COVID grants, and I presented that information to you all, and then you are deferred. It's a Compliance Committee to, I'm sorry not to PCC program compliance in order to determine the impact if any of the I of the the march 31 deadline on those grants. So that's and then the In addition, at the last meeting, there was a presentation of amendment to the procurement policy, and it was deferred or requested. It was passed with, you know, to go to policy. Policy got canceled, so I brought the list to finance. It'll also go to policy if you guys wanted as well. But because policy got canceled, I did bring that list of any grant, any contracts, between 50 and 100,000 because one of the request of this body was approve a change that board actions under 100,000 or but board actions over 100,000 come to to the board opposed to 50,000 so that document is included in This packet. You guys, I think, initially asked for one year, and I said I would provide two years. So there is a document and in the packet that details those board actions between 50 and 100,000
+2
ma'am, through the chair. The first item was, if, just, if you recall from the last meeting, this body asked me for an analysis of how much, which grant, which COVID funds, were impacted by the the federal cease of COVID grants, and I presented that information to you all, and then you are deferred. It's a Compliance Committee to, I'm sorry not to PCC program compliance in order to determine the impact if any of the I of the the march 31 deadline on those grants. So that's and then the In addition, at the last meeting, there was a presentation of amendment to the procurement policy, and it was deferred or requested. It was passed with, you know, to go to policy. Policy got canceled, so I brought the list to finance. It'll also go to policy if you guys wanted as well. But because policy got canceled, I did bring that list of any grant, any contracts, between 50 and 100,000 because one of the request of this body was approve a change that board actions under 100,000 or but board actions over 100,000 come to to the board opposed to 50,000 so that document is included in This packet. You guys, I think, initially asked for one year, and I said I would provide two years. So there is a document and in the packet that details those board actions between 50 and 100,000 Unknown Speaker
Okay. Do we have anyone to have any questions?
Speaker 4
I miss Black Mirror. Are we? Are we right now discussing with Okay, so when I look at this list of the 50 to 100,000 to go to 100,000 it makes you want to say, yeah, go to 100,000 what concerns me is not things like, Oh, the the camp therapeutic recreation or the accident fund insurance. Am I on the right subject? Yes, okay,
Unknown Speaker
I've done that before.
Speaker 4
I it. There's only one thing on here that I would would have wanted to ask questions about that would have been the consultant. What kind of safeguards would we have on going from 50,000 to $100,000 on
Unknown Speaker
I'm sorry, which, which consultant? Well,
Unknown Speaker
starfish family services consultant
Unknown Speaker
for 96 six so
Speaker 3
approved that that's actually a provider, not a consultant. I mean, I don't know if someone can speak to that, but starfish Family Services is one of our programs, one of our main, main, larger children's providers. This is one specific grant that they get. Okay,
Speaker 4
yeah, I'm thinking going forward. Okay, so, um, going forward, if we moved it from 50,000 to 100,000 everything on here, I would just as soon hand over to you and say you don't need to bother us with these sites, the only thing would be something like consultant. Is there any way to rule out personal service contracts or
Speaker 3
so that would come still come to you. It would just be in that quarterly report, whereby, right now is anything over under 50,000 come to you quarterly. It would then be changed to anything under 100,000 will come to you quarterly. So you it would get reported to this body, um, through that quarterly report. But I just want to note that this, this is that starfish is not a consultant. Okay, that's not a consulting contract mislabeled. Okay, yeah.
Speaker 2
Oh, anyone else? Dr, Tay, so just to, just to confirm it's not consultant. Is mislabeled? Or is it consultant? It because they could be doing some consulting services over and above their provider role. But I just need to clarify
Speaker 3
Good afternoon. This is Cassandra Phipps, relatives, initiatives. I just wanted to state that we have a contract with starfish and University of Michigan for the MC three program. And so that's what this program is for. What it is is they, they provide behavioral health consultant staff for this program. You repeat that, Cassandra, what is them? Behavioral behavioral health consultant. So it's for the MC three program.
Speaker 2
They asked about it last meeting. Yeah, but what is MC three? What does that stand for? It's
Speaker 3
not. It is where we it's in tandem with the University of Michigan. They provide psychiatric consultation to doctors that might need to consult with their medication, and then behavioral health consultants are housed in the clinics to provide consultation to those clinics. It's a federal grant that we receive from the feds that we contract with starfish. And I think she said, Wayne State, yes, okay, all right.
Speaker 5
Commissioner Kinloch, oh no. No questions. Thank you.
Speaker 1
Anyone else else have any questions concerning the contract or the request to have the contracts going from 50,000 to $100,000 threshold?
Speaker 4
Is there a way to segregate personal service contracts under keep that at 50 or no. I just know that, although I've got a very, very high respect for whatever you guys do in government, they hire people a lot, and they put the name consultant on it, and I know that that's not a consultant. But what would worry me is if somebody did hire somebody as a consultant, and we wouldn't know about it until such such times have done
Speaker 5
Mrs. Madam Chair, Commissioner, Ken lot, so, so what, what you're what you're asking is that for personal service contracts, or professional service contracts, that those still require Board approval under
Unknown Speaker
less than the threshold that we're, we're they're
Speaker 4
proposing. Let me ask you this, if it would be difficult to do that. I mean, doesn't sound like it would be difficult. You only, you only have one, and it's mislabeled. So
Speaker 1
you're talking about carve out that and leave that at the $50,000 threshold. So
Speaker 3
I guess I would ask, you know, historically, you know, as because I understand that there has, you know, in government, this has always been somewhat of an issue in terms of, I mean, I remember that back in the county days, right? I would just ask, I guess, since you've been on this board, has been a part of this body, has it been an issue?
Unknown Speaker
No, never has. That's why I have a very high so
Speaker 3
if it hasn't, I guess if so, if it hasn't been, then why would we think that it would it wouldn't bother
Speaker 4
me if I lost this argument, but it would it be difficult to do.
Speaker 5
Mr. McNamara, can we, since we're putting into place, we can always do at the Commission, we can always take a look at it in the future. If it becomes an issue to have the consistency in the policy, I think it'd be a good proposal.
Speaker 3
Yeah, and again, it'll it'll come you on a quarterly basis, so we'll
Speaker 5
be able to see it. And if we think it's an issue, then we can rate Absolutely. So you're
Speaker 6
Go ahead. Mr. Parker, when it comes to us in the core report is already done, information item not it's just information something that we can change. The question I have, are any of these? Or in the future, if a RFP goes out for particular, anything, commodity, service or whatever. Does that make any difference? Still, if it's under 100,000 it could be approved by administration not come to us?
Speaker 3
Yes. So also requested to be in line with this request on board approval. We're also requesting at the threshold for RFPs, for formal solicitations be also increased to 100,000 so if it is an RFP, it will come to you.
Speaker 6
Okay, if it's RFP, it does come to us, even if it's under 100,000
Unknown Speaker
No, no.
Speaker 3
So, so part of what was presented to this body last month was, along with the equalization credits and the things that you all had requested, in terms of, you know, county based and so forth, there were two things requested. One was that the Board approve contracts, instead of 50,000 it'd be 100,000 the second request was for formal solicitations are required over 100,000 opposed to 50. Right now the CFR, the federal guidelines, allow up to 250 for a non formal solicitation. We were only asking for up to 100 so things under 100,000 to be answer your question directly. Contracts under 100,000 would not require a formal solicitation. Contracts above 100,000 would require a formal solicitation, and and they would have to come to this body as well.
Speaker 6
So you're saying, when you do the solicitation, if it's under 100,000 you could make you could approve it without it coming to us. That is not an RFP, but just calling up three companies, and that's what their prices
Speaker 3
and getting its informal quotes and up to a reasonable amount, is what the CFR says. And generally we do three Yes, that is correct.
Unknown Speaker
And these are the ones that's been under 100,000
Speaker 6
but over 50 for the last did you say two years? Two years? Yes, it's not as many as I thought it was, yeah, it's
Speaker 3
not. There's a lot. That's why we are really kind of asking for it, because it's not a lot. It's just it helps.
Speaker 2
Thank you. Madam Chair, Madam Chair for me. Dr tag, so if a company in the course of a year requires two 100,000 or under 100,000 Would that then come to the board, or would it
Unknown Speaker
be this listed twice, um,
Unknown Speaker
you know,
Speaker 3
I believe that if it's a different scope of service, it's considered to be a different contract. So it could be more multiple companies with because I think it's based on contract and scope of service. So it could be a company that may offer a array of services, and if we contract with them for for a certain scope, and it's under 50, then they've got an offer another service that we contract, I believe, but I can get back with you. I believe that would be considered two separate contracts.
Speaker 2
Okay, just wanted to clarify and one, one other clarifying question with the plans that we currently have in place for expansion, do you expect this number to increase in any significant
Speaker 3
way? It very well could be absolutely, absolutely
Speaker 2
okay. We'll just have to watch it quarterly. I'm just, I'm just concerned that a lot of the things, but like Mr. McNamara, that things will come through that we aren't aware of, and maybe we would want to be aware of, but well, you would be,
Speaker 3
you would get aware of them, but to admit to Commissioner Parker's point, it would be after the fact, but they would come to your attention. And I mean, obviously, if it becomes something that you all find troublesome, then you you change your policy. Yeah. I mean, that's under you. That's your
Unknown Speaker
purview. All right. Thank you very much, Commissioner Ken lot.
Speaker 5
I know I'm not a member of this committee, but in the aggregate, can, I mean, can a pop this policy be amended, whether, at any, whatever policy need to be amended to say, any aggregate, if any of these companies, or any company to receive an aggregate, or whatever services over 100,000 if that triggers approval by The board? So regardless of, regardless of what the scope of services is, if this particular company is getting any aggregate awarded to the board, absolutely within that, within a 12 month period, okay, yeah, put that in there,
Speaker 6
and Mr. Parker, just as follow up on the one about, if there's a contractor that has two separate contracts that were coming like the ask them fund insurance company on America as a 54 and a 57 but everything else is exactly the same work on compensation insurance. So, you know, is that? So it looks like, as long as it's a different, I don't know what the term is different or something else, but it looks like they're both the same thing. Worker, conversation,
Speaker 3
different fiscal years, I think, pardon um, if you look at the first three of them in there, so if you look at the board, action, 25 dash, 36 and 24 dash, 24 so it's two different fiscal years, three,
Speaker 6
three years, I see you're just doing this as an example for 20. So it's not the same year that it was done in. It's
Unknown Speaker
not the same year. Thank you.
Speaker 1
So I you had a question Dr day, so I'm inclined to because that's where I was going with it. Commissioner Kinloch is just for, I guess, purposes to eliminate the
Unknown Speaker
possibility of multiple
Speaker 1
contracts or RFPs to individuals under the $100,000 threshold, but being multiple in a year,
Speaker 3
I would agree with the aggregate. We can, we can do that. We can add language that aggregate. That's not, that's not an
Unknown Speaker
issue. And I don't know if you do it for
Speaker 1
um, on an annual basis, the average for a fiscal year, the fiscal year aggregate of 100,000 to any individual company, yep, and or affiliates. I got it, yeah, any country in the any individual company and, or subsidiaries and affiliates, yes,
Speaker 3
that one may be a little bit because, I mean, they should kind of have to know who's a subsidiary of who that may be a get a little bit complex. Um, well, we can always, we don't. I mean, you have, yeah, we would have to look up everybody to see if they have
Unknown Speaker
to depend on them as right? They have
Speaker 1
to, if they, if they don't fail you, then you can't, you know, never know. They have to tell you, trust, inquire, or do we do any business with any other, any of your affiliates and or subsidiaries, and if they know, then you have a trust issue. If it's not, yeah, yes, just
Speaker 4
on that point, our contracts all fill out on Yeah, they fill out stuff saying, this really called a vendor conflict of interest form, I'm sure they do, right?
Speaker 3
Yes, they do. Fill out ethics form. I have to come, I have to take a look at it to see if it says currently, says affiliate, subsidiaries, etc. But we do, they do fill out an ethics form.
Speaker 4
I mean, I know the city of Detroit does. I know Wayne County does. If you're following their procurement, it must be all right,
Speaker 1
so we're good with that piece. Let me go back to the program Compliance Committee. You said we didn't have a meeting or it wasn't referred. Let's see the policy they got referred to.
Unknown Speaker
PCC,
Unknown Speaker
okay, okay,
Speaker 2
Madam Chair, if I may, Cassandra Phipps, Miss Phipps has her hands up and Mr. White has joined the call via zoom,
Speaker 1
okay, um, thanks for joining Mr. White and Cassandra. Your question. Yes,
Speaker 3
thank you. I just wanted to clarify. I know the formatting on the sheet, it makes it seem like it just says consultant, but the line right above consultant says Michigan collaborative care program, MC three and behavioral health consultant, yep, so I just wanted to make that clarification. It does say the full name on here. Thank you. Thank you because
Speaker 1
Thank you. I actually caught it after South Thank you.
Unknown Speaker
Thank you for that,
Speaker 2
Madam Chair. Do we need a motion as a recommendation or just goes to policy committee. How? What would we?
Speaker 3
Madam Chair has already been referred to policy committee. So when we discuss it at Policy Committee,
Speaker 2
and that will include a discussion of the amendment that we just made to the correct
Speaker 1
although that's the action item or follow up items that'll go to the policy as the recommendation from finance. It's already been referred to policy me, when they get ready to discuss it, it'll be either in the recommendation
Unknown Speaker
to them, if you would like, subsequent, subsequent,
Speaker 5
subsequent discussion should be sent to and
Speaker 3
also through the chair. It'll be a part. It'll we'll make amendment to the policy already operate that language,
Speaker 1
okay, I just wanted to make sure that it doesn't get lost, better than it will not get lost. Okay.
Speaker 1
Okay, so what can I get an approval of the minutes, please. So move or properly moved and supported? All in favor? Anyone opposed, any discussion, presentation of the monthly finance
Speaker 3
report,  ma'am, so presented before you as the monthly finance report for the seven months ended April 30, 2025 the first item that I wanted to bring to the attention of this board is that there had been a lot of discussion at supposed discussion at the federal level, that the HRA payment, or hospital rate adjustment payment that is a pass through from the the state to Detroit, Wayne to the hospitals, was actually at jeopardy of one of was one of the Medicaid cuts that were that was on Jeopardy. We got notification, I want to say, a couple weeks ago, that that, that, that not only was it not, is it not in jeopardy, the Feds did. CMS did approve their hospital rate adjustment, and they also increased the amount that the HRA payments will be. So just the refreshing the board on what an HRA payment is. It stands for hospital rate adjustment and what it does, it allows the hospitals to get additional compensation and to encourage and incentivize hospitals to take our members or Medicaid persons that are on Medicaid, because private insurance pays a lot more. So this is sort of to subsidize and give an incentive and additional funding to hospitals to take our members, so that that bill or CMS did approve that and they actually increased the payment. Good deal. So we there is a budget adjustment that is actually in this, in a board action to you all this, this, it's on the agenda later on, under old business or unfinished business, that will increase that amount. Where it's the estimate, the rate went up 20% so we figured that the funding will go up to 20% as well. So there is a budget adjustment that is before you all for approval. Good. I just want to highlight that, you know, there's, there's been a lot of, I don't want to say hearsay, but it's a lot of stuff going on at the federal level about Medicaid cuts and jeopardize and I just want to just point out that this was one of the ones that was, you know, there was discussion about that that actually did not get cut and actually got an increase.
ma'am, so presented before you as the monthly finance report for the seven months ended April 30, 2025 the first item that I wanted to bring to the attention of this board is that there had been a lot of discussion at supposed discussion at the federal level, that the HRA payment, or hospital rate adjustment payment that is a pass through from the the state to Detroit, Wayne to the hospitals, was actually at jeopardy of one of was one of the Medicaid cuts that were that was on Jeopardy. We got notification, I want to say, a couple weeks ago, that that, that, that not only was it not, is it not in jeopardy, the Feds did. CMS did approve their hospital rate adjustment, and they also increased the amount that the HRA payments will be. So just the refreshing the board on what an HRA payment is. It stands for hospital rate adjustment and what it does, it allows the hospitals to get additional compensation and to encourage and incentivize hospitals to take our members or Medicaid persons that are on Medicaid, because private insurance pays a lot more. So this is sort of to subsidize and give an incentive and additional funding to hospitals to take our members, so that that bill or CMS did approve that and they actually increased the payment. Good deal. So we there is a budget adjustment that is actually in this, in a board action to you all this, this, it's on the agenda later on, under old business or unfinished business, that will increase that amount. Where it's the estimate, the rate went up 20% so we figured that the funding will go up to 20% as well. So there is a budget adjustment that is before you all for approval. Good. I just want to highlight that, you know, there's, there's been a lot of, I don't want to say hearsay, but it's a lot of stuff going on at the federal level about Medicaid cuts and jeopardize and I just want to just point out that this was one of the ones that was, you know, there was discussion about that that actually did not get cut and actually got an increase.
+1
ma'am, so presented before you as the monthly finance report for the seven months ended April 30, 2025 the first item that I wanted to bring to the attention of this board is that there had been a lot of discussion at supposed discussion at the federal level, that the HRA payment, or hospital rate adjustment payment that is a pass through from the the state to Detroit, Wayne to the hospitals, was actually at jeopardy of one of was one of the Medicaid cuts that were that was on Jeopardy. We got notification, I want to say, a couple weeks ago, that that, that, that not only was it not, is it not in jeopardy, the Feds did. CMS did approve their hospital rate adjustment, and they also increased the amount that the HRA payments will be. So just the refreshing the board on what an HRA payment is. It stands for hospital rate adjustment and what it does, it allows the hospitals to get additional compensation and to encourage and incentivize hospitals to take our members or Medicaid persons that are on Medicaid, because private insurance pays a lot more. So this is sort of to subsidize and give an incentive and additional funding to hospitals to take our members, so that that bill or CMS did approve that and they actually increased the payment. Good deal. So we there is a budget adjustment that is actually in this, in a board action to you all this, this, it's on the agenda later on, under old business or unfinished business, that will increase that amount. Where it's the estimate, the rate went up 20% so we figured that the funding will go up to 20% as well. So there is a budget adjustment that is before you all for approval. Good. I just want to highlight that, you know, there's, there's been a lot of, I don't want to say hearsay, but it's a lot of stuff going on at the federal level about Medicaid cuts and jeopardize and I just want to just point out that this was one of the ones that was, you know, there was discussion about that that actually did not get cut and actually got an increase. Speaker 1
Good deal. Anyone have any questions? Mister Parker, there's
Speaker 6
a question on that. I mean, I noticed what they call it the beautiful budget, or whatever, beautiful don't cause it, is it included in there in any
Speaker 3
way? Um, I'm not certain, not certain. Thank you. The next item is so throughout the year, I have to submit reports to the state on projections on where we're where we're at, based on our, you know, revenues and activities and costs and utilization. So we had a mid year report that was due literally on Friday. And based on that mid year report, dwin was looking at a shortfall and Medicaid shortfall. So our utilization costs were exceeded our revenues by about $30 million dollars. That $30 million was going to have to come out of our $70 million internal service fund, obviously still leaving $40 million in the fund. But something that you know was, was would have been of to keep our eye on and be very watchful of, right? So literally, on Thursday, when I was submitting this report or gotten all the information together to present to you, we got a rate adjustment letter from the state of Michigan, um, whereby they are amending the rates and they're adding an additional 140 $8 million to the system because of higher utilization and cost. So the same thing that we were experiencing as a result of that, you know that 30 million the state saw it sent a rate letter on literally, on Thursday, literally, I had to literally change this report. I was about to send this a Lillian, but they're going to disperse $148,000 and I estimate the dwin will get at between 30 and 32 million. So we're hopeful that that all comes to fruition, and we won't be able, we won't have to use our ISF to the degree that we thought that we would had. So I just wanted to pass that information along. That's pretty good news, and it was right on time. Good
Unknown Speaker
deal. Are there any questions?
Speaker 1
So the state of Michigan gave us a state adjustment, adjustment,
Speaker 3
they're doing us a rate adjustment. And the funding will get distributed July, August and September, so that additional 30 million will come through, July, August and September. So the state seeing the increase in utilization, it's across the state. I mean, we're certainly out of out of COVID, for sure.
Unknown Speaker
The next item number three,
Speaker 3
you know, if you all remember, at the end of fiscal year 24 we had a general fund shortfall. We are projecting that we're going to have a general fund shortfall again, to the tune of approximately $12 million I can say that our local revenues, our current year, local revenues, will be able to cover that deficit without going into reserves. But we, we are seeing at least a 20 $12 million it's around $12 million
Speaker 4
but it's our current local revenue reserves. Sherman,
Speaker 3
our current local revenue reserves is $74 million thank you. 74 million but, but, but this, we have enough local, local revenue to cover it in the current year. With the current revenue, it won't come out of the resource. Won't come out of reserves. That's correct. Can
Unknown Speaker
you? Can you? I have a I'm sure one of you ask
Speaker 2
Dr tag, is there any one area that, or what's the majority of this shortfall from, or what's the what's the main part? And I'm just thinking ahead and wondering if it has, if it has implications for us to adjust our general revenue, budget, spending, but in any case, please answer that question,
Speaker 3
yeah, so it's a lot of it is coming about due to one spend down, and secondly, getting people back on Medicaid quickly during their redetermination period. It's taken, it's taken time. We've put some skin in the game, if you will, for providers to because before, you know, prior to this, providers still got paid regardless. So there was no skin in the game to make certain that, you know, you know, Stacy, you know, needed to turn in her bank statement in order to get her Medicaid turned back on in timely fashion. Well, you know, Stacy took three months to do it. And guess what? The providers kept getting paid regardless of Stacy, you know, being maybe in a residential home where the residential provider is seeing them every day, but Stacey, you know, the residential providers still getting paid for their services. And Stacy needs to turn in the bank statement, and it's taken me three months to do so. So now there are, there is some skin in the game where it incur it basically it incentivizes providers, and if they want to get paid that, they need to get Stacy's bank statement in to the DHS office in a timely fashion. Okay, just
Speaker 2
a follow up question, if I may, Madam Chair, to the chair so my recall correct me if I if it's if it's wrong that we are the only agency that that pays to spend down.
Speaker 3
Oh, no, no, no. Others do it too. Oh, absolutely, all right, absolutely. If we didn't pay spend down, we would have it would it would come. It would come out of members SSI chair, gotcha. And they don't, absolutely, it comes, I think you have to come out of members, whatever social security payments that they receive. So yes, I'm not aware of any CMH that does not pay spend down. It could be somebody out there, but I'm not, I'm personally not aware of any. Thank
Unknown Speaker
you. That's a good thing to do. That absolutely.
Speaker 6
Mr. Parker, that was the same line of questions I wanted our chairperson.
Unknown Speaker
Do we have any run online question?
Unknown Speaker
Who's joining us online?
Speaker 3
Mr. White, and then there are some staff members that are joining Madam Chair,
Unknown Speaker
Mr. White. Then that's close.
Speaker 3
Go ahead. Okay. So the next item is that mdch announced that, effective October 1, 2025 that they will be directly managing the payment and the oversight for all ccbhcs. What does that mean for us? Okay, what does that mean? We've got seven ccbhcs providers in our region right now, and they're there. There are two parts to the payments that we pay ccbhcs. There's the Medicaid base payment, which is part of our capitation Medicaid capitation payment, and then there is a supplemental payment, which is money the state gives to us that we pass through to them, so it's passed that's passed through Monday, okay, so that that pass through will go away the Medicaid. Based on the Medicaid base, we're estimating that the Medicaid out of the billion dollars. And I want to keep this in perspective for everybody, right out of the billion, out of the billion dollars that we receive in Medicaid, 50 million will be carved out. And I estimate the 50 million would be carved out, because that's really where the concern is, is making certain that they calculate what that carve out piece is, right? But I estimate the 50 million of a billion will be carved out, and the state will retain that to pay the ccbhcs directly.
Unknown Speaker
That sounds
Speaker 3
so not only will we not have the revenue, I just want to be clear so we won't have the revenue, but we won't have the expense either. Okay,
Speaker 4
Mr. McNamara, so it's only each CTB, HC is only estimated to affect our bottom line by $7 million
Speaker 3
No, no, it's affecting our so our budget, if I, you know, after, if I were to, you know, redo our budget, I would take off $100 million of our budget. Oh, okay, so it's 100 million. It's 50 million of Medicaid, and then another 50 million of pass through supplemental,
Speaker 4
okay, and how much the pass through is our administrative fee? 400,000
Unknown Speaker
Okay, okay, let me take that back. About 600,000
Speaker 4
I would just worry every time I hear CCBHC I keep on, it's about six these guys could gut us within days, it seems. But it doesn't sound like it's going to happen at all.
Speaker 3
That is not going to gut us. I mean, like I said, I want to just keep it in perspective, we got a billion dollars in
Speaker 4
Medicaid. It sounds it's wonderful news. Thank you. It sounds a little worse
Speaker 1
than what it is, you know. So what you're saying, essentially, in a nutshell, that 600,000 is what we'll lose out on as it relates to fees. That's correct, okay, Dr tag. And
Speaker 2
also, we do have ccbhcs. I know we're still waiting for the federal approval, but we still will get some money back just because we have a CCBHC. Is that correct?
Speaker 3
So if I understand the way it works, is that if we were a CCBHC, the Medicaid and the supplemental related to dwin as a CCBHC would come back to us, perfect, yeah, directly from the state, which it does already, right? Anyone?
Speaker 1
No, you're good. Any other questions
Unknown Speaker
proceed. Madam CFO, okay,
Speaker 3
so, and the last item is that on May 29 our cash collateral that was held for our construction was released, and I did transfer that into our main depository account so that funding that that cash is now available for disbursement amongst the provider network. Good deal. Mr.
Speaker 2
Walsh, can you tell me what that amount is? Please, the amount that is being
Speaker 3
the amount is the amount we transferred was around 20 million. 2 million remain, 2,045,000 remained as restricted, because, if you recall, that was the difference between the second appraisal we got on this building and what the and what the loan amount was. So 2 million stays restricted, but they released 20 million. So 20 million got transferred around 2021
Speaker 1
Thank you. Any other questions
Unknown Speaker
you're done with your report? Well,
Speaker 3
unless there's more questions that does conclude my report,
Speaker 4
Mayor, can we go to the section C the Ibn R payable? Yes. So every month there appears to be a larger and larger growth in that area. Does it ever get cost settled with the state, where they just basically grabbed that 94 million or
Speaker 3
so? So Ibn R stands for incur, but not reported. It's very common in a claims based system, a healthcare system, that you've got claims that have and services that have been performed, but we haven't gotten a bill yet.
Speaker 4
But the point of the matter is, is every month that number goes up, so sooner or later, somebody's gonna say, okay, that service was, was never performed. We over, we over paid DWIHN Who didn't overpay the client. Yes,
Speaker 3
that never happens. That's not, that's not the way. So, so
Speaker 4
then you and I don't want to take up his time, but maybe you can explain that to me a little better some other time. Absolutely okay. I don't get it.
Speaker 3
It's an estimated amount based on past claims, actual
Unknown Speaker
billings or past claims, past claims.
Speaker 3
It's an estimated amount based on past claims and what we have paid as of a certain period in time,
Speaker 4
but at but every month that number goes up.
Speaker 3
It could be an indication of, you know, timing and when providers are submitting, you know, their their their claims. It could be a factor of increased utilization, which is what we are seeing, is increased utilization, but it's,
Speaker 4
it can't be a factor of the fact that they are not that they're not producing as many services as we're estimating that they are producing. Say that again, basically we're claiming they did $94 million worth of work that they haven't built as far that's correct. Okay, did? How do we know that they did $94 million worth of work that they
Unknown Speaker
didn't bill as far as an estimate? Okay,
Speaker 4
that number was 50 million a year ago, and it went to 60 million, then went to 70.
Speaker 3
Now it's at 90 again. It is based there. I'm just wondering
Speaker 4
if this anytime the state steps in and says, Okay, you got to readjust this
Speaker 3
back. Oh, this has everything to do with me reporting the financials and making certain that they are materially Correct. Okay, this is, it's an estimate. And, yeah, no, the state doesn't come and say, you know, we want that money. No, that, that's not the way it works. It's an estimate. All right, if I didn't put it there, it would show that we had 94 extra million dollars.
Speaker 4
Well, that's revenue. Later they're going to ask, I mean, I know you've got that money invested, because you're pulling down $6 million a year in interest. And I'm like, Are they gonna grab that
Speaker 3
now that that eventually runs its course? So at the end of the fiscal year, it we report with everything. So at the at the end of the fiscal year, everything for the fiscal year gets reported. So you don't have that, that if you, if you looked at financial statements at the end, at our on our audit reports, you're not going to see an Ibn R, payable, um recorded, because we, we report everything. By that time the statements get issued, everything's been reported to us. Oh yes. Thank you. Yes.
Unknown Speaker
Okay, absolutely. Thanks.
Unknown Speaker
No questions now.
Speaker 1
Any other questions concerning the finance report? Okay, thank you. Would like to receive and found the monthly finance report, fiscal year 26 budget submission. Timeline,
Speaker 3
yes, 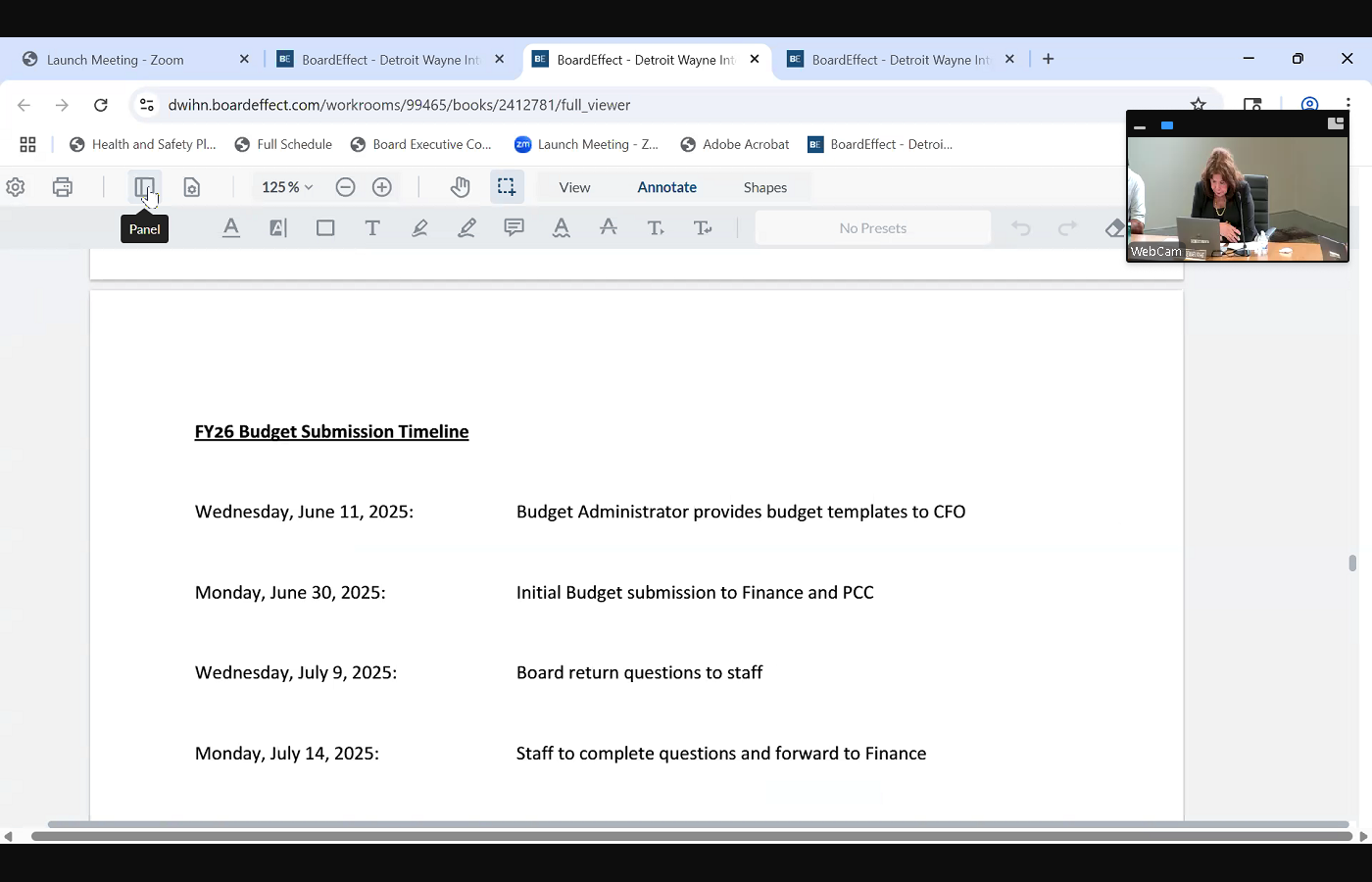
 so through the chair on an annual basis. As you all know, we have a joint PCC and finance committee meeting the first Wednesday in August. That would be August six, based on the calendar, the timeline would be that the we would submit give you give the board the initial budget packet on June 30, you would give us back and return any questions by the ninth, and then we would give you a final board packet, including responses to any questions that you proposed by Wednesday, July, 23
so through the chair on an annual basis. As you all know, we have a joint PCC and finance committee meeting the first Wednesday in August. That would be August six, based on the calendar, the timeline would be that the we would submit give you give the board the initial budget packet on June 30, you would give us back and return any questions by the ninth, and then we would give you a final board packet, including responses to any questions that you proposed by Wednesday, July, 23
+2
so through the chair on an annual basis. As you all know, we have a joint PCC and finance committee meeting the first Wednesday in August. That would be August six, based on the calendar, the timeline would be that the we would submit give you give the board the initial budget packet on June 30, you would give us back and return any questions by the ninth, and then we would give you a final board packet, including responses to any questions that you proposed by Wednesday, July, 23 Speaker 1
Okay, any questions concerns.
Unknown Speaker
Thank you.
Unknown Speaker
Unfissioned business. Board action 2525
Speaker 3
Yes, 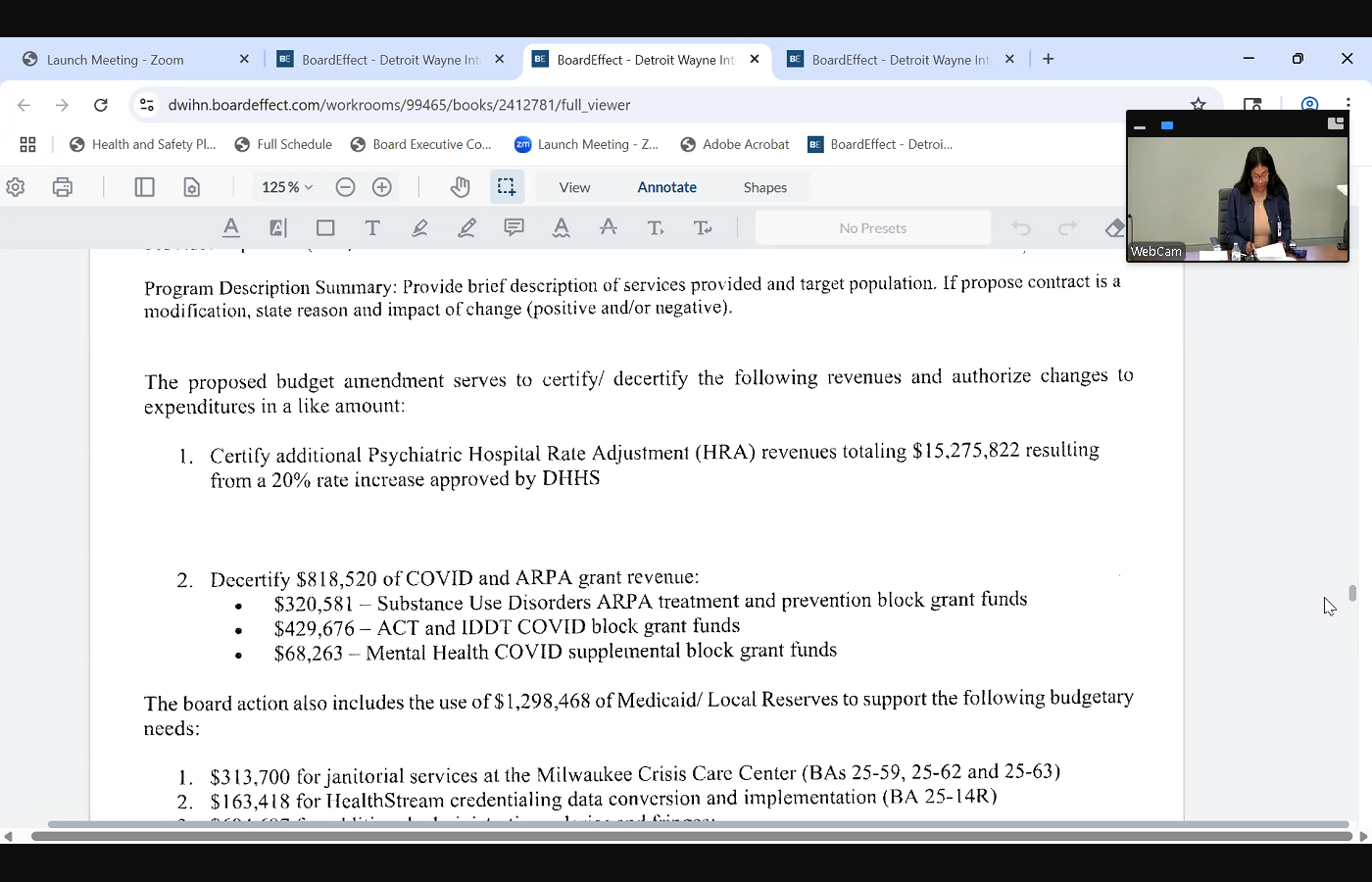
 board action 2525 is the budget amendment that we spoke about in regards to HRA, where we are certifying an additional $15.3 million related to a the anticipated HRA increase resulting from a 20% rate increase that was approved by DHS. In addition to that, we're decertifying $818,000 for the COVID and ARPA grant revenue that had that ended on March 31 and in addition to that, we're including additional Medicaid reserves of 1.3 million related to approximately 314,000
board action 2525 is the budget amendment that we spoke about in regards to HRA, where we are certifying an additional $15.3 million related to a the anticipated HRA increase resulting from a 20% rate increase that was approved by DHS. In addition to that, we're decertifying $818,000 for the COVID and ARPA grant revenue that had that ended on March 31 and in addition to that, we're including additional Medicaid reserves of 1.3 million related to approximately 314,000
+2
board action 2525 is the budget amendment that we spoke about in regards to HRA, where we are certifying an additional $15.3 million related to a the anticipated HRA increase resulting from a 20% rate increase that was approved by DHS. In addition to that, we're decertifying $818,000 for the COVID and ARPA grant revenue that had that ended on March 31 and in addition to that, we're including additional Medicaid reserves of 1.3 million related to approximately 314,000 Unknown Speaker
for janitorial services,
Speaker 3
for both the for the care center. 163,000 for health stream, credentialing, data conversion and implementation. 694,000 for additional administrative salaries and fringes. And there's a detail of what the six, 694 694 represent. In addition, there's 126,000 in salaries and fringes for for new contingent, mobile crisis positions,
Unknown Speaker
maybe one anyone have any questions?
Unknown Speaker
So these are, oh, Mr. Parker, yeah,
Speaker 6
just the additional administrative salaries. Is that all pertaining to the care center? No,
Unknown Speaker
um, administration staff.
Speaker 3
So I can tell you that the the facilities and the HR positions pertain to direct services, and the fact that, you know, we've got the buildings, and you know we need additional staff in order to, you
Unknown Speaker
know, continue hiring,
Speaker 3
but I think the rest of them are regular administrative salaries or administrative cost.
Unknown Speaker
So these are not anticipated when the budget
Unknown Speaker
made last year. That's correct.
Speaker 6
This is actual amount that we're need to have spent,
Unknown Speaker
roughly half 700,000
Unknown Speaker
That's correct.
Speaker 1
We have any other questions as it relates to the budget. I have a question Miss room, so
Speaker 7
I'm just curious. I know this is a Jodi question, what are the three new facilities positions, and then what are the new contingent mobile crisis positions is for?
Speaker 3
So I know with the mobile crisis positions, I believe it's because there is a lot of overtime being incurred. So we wanted to bring in additional staff to really reduce the amount of overtime. But I'll let others speak to and again, you know that it says contingent. So contingent is, you know, in the event we need them, then we call upon them. But it's directly, I believe, to address the overtime related to staff.
Speaker 8
Good afternoon. Mike baski, Executive Director facilities, the positions that we have posted are going to help accommodate all the new contracts that we have coming forth with the facilities. Now that the facilities warranties are starting to expire, we have a tremendous amount of contracts that we're going to be executing, as well as inventory and fleet management. Now that we've got mobile crisis fans. We need individuals to help service those and keep them on the road, making sure tires are rotated, oil changes are completed, things of that nature. It just helped the department come become more efficient.
Unknown Speaker
Saying one of them is like maintenance of vehicles. That's what I heard you
Speaker 8
say. It's just a person that will coordinate it all make sure that it's completed. There's there's three positions there. There's contract management, vehicle, vehicle and fleet management, inventory management, that's included with those positions. Like the care center, we have to have so much percentage of materials on hand for maintenance, whether it be light bulbs, you know, plumbing, parts, things of that nature, we need someone to help manage and make sure that those parts are on hand at all times. So the service tickets that we get at the crisis center, we average roughly on a seven day week. We average three to four tickets a day just at the crisis center for repairs. And we need to make sure that those materials are on hand.
Speaker 3
And if I can add also making certain that the vehicles are gassed up. And we we don't want to pay conditions to gas up the time spent gassing up on vehicles, because we want them to be clinicians, right? So this person would also be just make certain the vehicles are fueled, washed clean, so that members are getting into and we're presenting a good front, and members are getting into clean vehicles.
Speaker 7
So it's like a dealership Porter, basically. It sounds like a dealership,
Speaker 8
essentially, a little bit more responsibility than the general Porter, but yes, okay,
Speaker 7
you said it okay. You said three. But on here, it says four.
Speaker 8
I'm sorry. Position, yeah, there's four in total. Yes, I misspoke. Okay,
Unknown Speaker
the three facility. There's three facilities.
Speaker 8
There's three facilities. I think you said four positions in
Unknown Speaker
these days. No, it's two.
Speaker 1
That's two different things. There's four for the mobile crisis. Yes, four. Okay, yeah,
Unknown Speaker
it was three for me. I'm sorry. Okay, all right,
Unknown Speaker
Jodi, but
Unknown Speaker
you making sure you fumble?
Speaker 1
No, I, I Okay. I was here to answer any questions that well, you're on Go ahead. Yeah, I'm up here. So there are, there are two human resources, generalist positions that are also being requested due to the significant increase, significant increase in staffing. We need these additional positions in order to support HR needs for the additional staff.
Unknown Speaker
And I hear something. I hear,
Speaker 2
Mr. White, do you have your hand up? I
Speaker 9
did. I just wanted to, I just wanted to add a little bit more to the request for the contingent employees at the crisis unit, as indicated. The primary reason for that is just to have the availability of staff as well as to reduce the overtime. So they have literally on standby. As the board is aware, we've, we've, we're coming up on our one year of utilization of the crisis services unit, and we're looking at, you know, 2000 runs that they've handled so and the numbers are expected to grow over the summer, so that staff is very much needed. And with regards to the the vehicle maintenance, the other big responsibility is just maintaining the mobile clinic, which is a significant responsibility, from cleaning it to making sure that you know it's ready to go when we roll it out throughout the community, so that that position would also incur those responsibilities as well. Thank you.
Speaker 1
Any other question as it relates to literature, you have a question, doctor. I mean, I'm sorry. Mr. Walsh, yes.
Speaker 2
With regard to the positions that you're requesting, the increase these have to be filled by September 30, correct?
Speaker 3
Yes, yes, I think they're trying to fill them now. I'm not, yeah, they're trying to fill them now,
Speaker 2
right? I only ask because it's only a few months away, and that was, you know, why I was asking, if you don't feel the positions. What happens with the
Speaker 3
and they, they be, they, they'll be on our fiscal 26 budget. Okay, they'll get filled.
Speaker 2
Okay, all right, thank you. That was big question through the chair. So you would just reallocate those funds, or would that become unspent funds? I
Unknown Speaker
i Say that again. So
Speaker 2
if they're not filled, then the funding that's allocated here for them would not be used. So what happens to those funds? Is it considered unspent? Goes back to the state, or do you reallocate it?
Speaker 3
No, no, we don't reallocate it, as you know, we're using reserves, so we just won't we will use less reserves,
Speaker 2
right? Oh, that's right, it is reserves. Thank you.
Speaker 1
Any other questions related to board action 2525 revision for
Speaker 2
Mr. Walker, one real quick, you did you say the amount of the increase? The difference between last year's budget and this year's from 1.5
Unknown Speaker
1.1 1.2 to 1.3
Unknown Speaker
is about what 100
Unknown Speaker
million or
Unknown Speaker
can you tell us what the increase is, the amount
Unknown Speaker
the for the salaries and no no for
Unknown Speaker
the entire budget modification. Okay, so
Unknown Speaker
hold on, it's,
Speaker 3
it's one point. Is 15 point 3 million for the HRA. It's a reduction of 808 million 808,000 for the decertification of the ARPA and COVID grants, and then there's an increase of our utilization of reserves of 1.3
Unknown Speaker
Okay, Thank you.
Unknown Speaker
Any other questions approximately 15.8 Okay, thank you.
Speaker 1
Any other questions relates to board action? 2525 revision four,
Unknown Speaker
board members, what's your pleasure?
Speaker 1
Support? Properly moved and supported. All in favor, aye? Anyone opposed? Any abstentions, any further discussion. Okay, new business, we have none. Or do we? Okay, okay, yes, Mr. Parker, I'm
Unknown Speaker
wondering, and I don't know if we have
Speaker 6
have enough information, so I'm just asking the question, you know, we the care center is pretty much operating now for almost a year. And I wonder, is there any analysis now of how much we've been able to reimburse versus the cost that it's costing us to operate the center, because we get reimbursement on a basis of the participation clients. But our costs are somewhat standard as far as personnel and cost of the building. So you're wondering where we're at. And again, I know we had not operated for a year, so you may not have that, but I'm just wondering if we're billing enough to pay for our costs.
Speaker 3
So you know, it's funny, but because we don't bill for our services, right? So we receive a capitated amount of funding that we get from the state, and we have to serve, pay providers, you know, administrative costs, everything needs to is a part of that capitation. So I'm going to use the term we eat off of one pot of money, and that includes the care center. So there is no billing. We don't bill the state. We we eat off of that capitated payment from the state.
Speaker 6
Okay, capitated, I'm just wondering if we're generating enough expenses when I was a capitation that equals the amount that we're putting into it. I mean, we're spending 3, $3 million operate the center a month, or whatever it might be, but we only have enough people that would capitation that would be 2.5 million. You know, is there any analysis like that? I just wonder how the care centers function. Well,
Speaker 1
you so, so, so that I'm clear, I'll make sure that I understand what you're looking for. You're just looking for, how, how? Basically, a wellness check on how the crisis center is doing. Like operates financially. What does it look like? Are we putting more into it then we're, you know, our what type of how is it affecting the budget? You see what I'm saying not a deep not is the crisis center, like, like we were talking about autism, autism costs are going through the roof. We know that autism is a big issue. So what he's saying is, is the wellness of the crisis center. How is that affecting the budget? Is that what I'm hearing you say?
Speaker 3
So the difference with autism? No, I mean, I'm not preparing out to providers so I can quantify how much we get in and I can quantify how much that goes out. The Care Center is a little different, but I think I'll hop Mr. White
Speaker 9
so through the Chair, I know exactly what you're asking. I asked the same question when I constantly and this capitation issue for me, is one that's quite confusing, that we start with a anticipated amount of usage, and those those numbers flow up and down based on a number of different things, from utilization to really hospitalization, number, number of different things, recidivism. So it's a complex issue. So I asked it at a very basic level, are we losing money? And the answer to that is, maybe it's a quite expensive endeavor. I'm very interested in that because I want to know what it's going to look like when we get to 707. Are we going to have a big empty building? Are we going to have a big field building? That's but it's not a money making endeavor. It's as you aware, it's a break even endeavor. I can honestly tell you that what I have learned from this process, we are not breaking even right now, but I will. If you give me some time to understand it myself more, I'll bring you a more complete answer. But I spent a lot of time with Stacy on that very issue. That's why I laughed and and I asked her the exact way did you ask? Like, are we losing money? You know. And she quickly was came to me with this capitation complex issue, but I'm very interested in it now. Here's what I do. Know we are running a delta at if we were to open up 707. Right now. And, e course right now you are looking at roughly absent any of the capitation issues, and reconciling those numbers. I see it as roughly a 30 to $36 million deficit that we're working through. But I haven't sounded the alarm yet because I need more background information to understand the reconciliation process. And
Unknown Speaker
if I can, well,
Speaker 6
we're getting the information later. I just think at some point we need to hear exactly what is happening.
Speaker 3
I think I can say, though, in terms of utilization and occupancy, right? Yes, in terms of that the adults are doing. I mean, they the beds stay full. I mean, it's over 100% like the adults, they are. They they jamming. I'm gonna tell you, they are jamming. The Children's is a little bit slower, and it's a little bit more of a struggle to keep the beds completely occupied. But adults is, I mean, is over 100% utilization
Unknown Speaker
and the and the funds
Speaker 1
we receive funds for the services that we render at those facilities, just as if we were a provider or No, no, Okay,
Speaker 3
we don't get funds as though we were a provider, and that's why that because Mr. Mr. White has asked that same question that Mr. Parker asked, you know, and it's not, we don't, we don't bill we're, we are the insurance company, right? We don't build the insurance company because we are the insurance company, right? So if you kind of look at it that way, so the funds that we use is part of Medicaid capitation. Thank you. Okay, yeah, okay,
Speaker 1
okay, so the Medicaid and that that is calculated, right? Yep, based on the rate. It's based
Speaker 3
on a rate times the type of Medicaid member eligible. Medicaid eligible member
Speaker 1
members, yes, right. So based on the Medicaid eligible members, yeah, and the people that we have in the that qualify as a Medicaid member,
Speaker 3
right, yep, the number of Medicaid eligibles, yep, right. Times the rate times the rate equals our capitation. It's
Speaker 1
right. So that's the only way that you can measure technically, right? Yeah, is based on that number. That's it. I can't that's right, right? But so if you got that number, and then the people that you're servicing. That's you. I'm just saying. I'm just getting to trying to figure out a way for you to really know what you're doing. You said. I'm saying because if you're you're getting your funds based on that rate, right? A rate
Speaker 3
times number of Medicaid persons enrolled in Medicaid, not how many members we serve? No,
Speaker 1
no, no, no, no. Right I get because, because, because the people that you serve that aren't enrolled in Medicaid aren't a part of that, right? Your Medicaid capitation rate, right? Yes, if they're not enrolled in if they're enrolled in Medicaid, right? So you're not necessarily getting anything from that correct? We want to get them enrolled in Medicaid, right? But service wise, you're not getting anything. I'm not getting a capitation. You're not getting anything for them. You're you're basically providing a free service. Well, not for general fund. General funds is utilizing those Yes, so you're not getting anything. You got that money. Your general fund is used that money. So the only way you can, I'm talking myself through this, so the only way that you're able to see would be how the measurement would be, how much of your general fund dollars you're using outside of that.
Speaker 9
And maybe because I've gone through this exercise so many times, I think an easier way for me to digest it was, you're absolutely right in terms of Medicaid eligibility versus the number of people you that are utilizing our services, right? But there could be and there will be people who don't have Medicaid that are using the services, we don't turn anyone away, right? But what happens over time with that medical or that eligibility, that Medicaid eligibility, is, if you are serving more people, then this recalculation occurs where you get a better slice of the pie, if that makes any sense, if they're Medicaid eligible, if they're Medicaid eligible, but they're not. There will be times when you you you engage, and you know what that percentage is of people who are not, and I mean that based on what happens over the next year, that that number could change, but there will always be some degree of people who are not Medicaid eligible that are getting services. So I think annually we will, we look at, essentially a recalculation of those who have access for services. And if the math continues to play out, and we do increase, and we're not seeking to increase, we want to provide if you need it, and naturally, if you had 2000 in one year, and you're getting ready to open up another center, you're going to increase. So I would hope. And as Stacey has not assured me, but certainly explained to me, that once the state looks at those numbers and that recalculation occurs, that's when the numbers should come into balance. But there's no guarantee,
Speaker 3
because other PIs, because remember, the pot of money is the pot of money, right? So it just gets redistributed amongst the pihp so, you know, if other pihps are increasing their utilization in the same respects that we are, then exactly. I mean, because the pot is the pot,
Unknown Speaker
pot is the pot. That's right, did that
Unknown Speaker
help anybody? I understand
Unknown Speaker
that? Oh, Mr. Walsh, I wash,
Speaker 2
so when we put together the funding for this project, didn't we have to put together a performer
Unknown Speaker
that would indicate,
Speaker 2
based on the funding that we're spending, this is how much revenue will be coming in, like, every month, or something like, No, you didn't. It's not,
Unknown Speaker
not, we don't.
Speaker 3
Oh, this is so hard to explain. We got it. We get a pot of money, and we, we have to serve we have to do everything with that pot of money, be every everybody eats off that pot of money, including that care center. We're at the point where, luckily we were, we were including the care center, everything. We were going to experience initially, a $30 million deficit, right? That's not going to happen, because they, they, they in, they put more money in the pot. Okay, so the pot of money that they at the top went up by 150 150 million. So we're going to get more. But that pot is we everyone eats off of that pot. This in the dwin network, including dwin, eats off of that pot of money.
Unknown Speaker
So then my second question is,
Speaker 2
with any new project, there's always going to be a period of one or two or maybe three years before you break even, I would, I would think, because you're starting something new, you know, you have to recruit, you have to bring in, enroll people. So there may not be that you know that performance the first year, maybe not until the second or third. So that was my other comment, more than anything, thank you. Mr.
Speaker 4
McNamara, yeah, I remember the discussion was, can we divert patients from hospitals, cope and things like that, and provide a more stable environment that was more cost effective? And I believe that we are, aren't we okay? So that was, that was what we were registering again. We also talked about a long time ago, whether or not we were going to try to find out at these patients at private medical insurance. Do we do that? I know that a lot of them don't, but I was, I remembered the hospitals scenarios. Many of them did. Is that part of the inpatient process
Speaker 10
to the chair for me? Yeah, I think, Mr. Parker, if I'm understanding your correct question correctly, you're talking about the coordination of benefit correct to ensure that Medicaid stays the pair of last resort and we exhaust all other billing insurances before Medicaid is you say
Unknown Speaker
it better than I would.
Speaker 10
So to answer that question, we do capture that information. What that requires is, it requires the clinicians to be credentialed with all those health plans for that specific population. In order to build those entities. There's a good news to that end. As part of our visit to natcon, we are able to engage with several entities who basically do this for business, in terms of getting provider organizations and peer organization credentialed, including crisis stabilization units, credentialed with health plans. We are in process of taking that up and ensuring we leverage even though it's a smaller population, it's not like our majority of population are walking in. I just want to make sure that it's not like we we are ignoring it. Majority of population is either uninsured or Medicaid. That's population itself. But I do want to state that there is a small population, percentage population, that do have a private pay. We are handling it two fold. One is and I don't want to digress away from CSU, but I will pick an example of ABA. We came across a certain population as part of a provider transition that had private pay. So we enforce our policy of ensuring that that coordination of benefit is attached to every claim that's coming from that specific provider before that gets adjudicated by dwin team to pay for Medicaid funds. So those kind of things and checks and balances are in place as income. As it comes to CSU, that's something we are in process of working to get providers, practitioners credentialed with all health plans that are applicable, so that in future, as we open our other facilities, we have a better attuned system in terms of navigating through the coordination of benefit. There are
Speaker 4
also companies out there that that work with fire departments, at least for crisis intervention and mobile crisis intervention, since you're getting into that world so but I'll just stop there. Thank you.
Unknown Speaker
Anyone else? No, all righty,
Speaker 1
good meeting, good discussion. We'll move forward to do we have anyone online Trent that would like to make remarks at this time, we would like to invite anyone online to raise your hand and for public comment. The welfare public comment. Do we have anyone in the room from the Public Good
Speaker 6
afternoon? Madam Chair, we did not receive any written submissions to public comment. There is no one in the room who wishes to make public comment, and none of our guests on Zoom raised their hand to make public comments so we have no public comment
Speaker 1
today. Move for adjournment. Thanks. Report properly. Move and support it. All in favor. Aye, anyone opposed want to talk about it? Thank you. All right. Looks like RIGHT.
Unknown Speaker
Anybody kind of radar tell me
Unknown Speaker
recording stopped.