Loading...
ICS Masterclass: Sacral Neuromodulation or Botulinum Toxin for Refractory OAB
Speaker 1
Good  morning. Good afternoon. Good evening, wherever you're you are around the world. And Howard Goldman and I'm very happy to welcome you to this ICS state of the art presentation. Who, what, when and why? sacral neuromodulation or botulinum toxin for refractory overactive bladder. I'm from Cleveland, Ohio in the United States. And I serve as the chair of the ICS education committee. So we have a really excellent presentation set up we have an outstanding faculty. All of our faculty members are experts in functional urology and have a lot of experience both with sacral neuromodulation and botulinum toxin and other therapies. So we're lucky we have a shiny Cashman from Adelaide. Australia. Dena Ultraman from Toronto, Mary and may petawatt. Vetter from not in France. I hope I pronounced that even partially right and rude. So hi from London.
morning. Good afternoon. Good evening, wherever you're you are around the world. And Howard Goldman and I'm very happy to welcome you to this ICS state of the art presentation. Who, what, when and why? sacral neuromodulation or botulinum toxin for refractory overactive bladder. I'm from Cleveland, Ohio in the United States. And I serve as the chair of the ICS education committee. So we have a really excellent presentation set up we have an outstanding faculty. All of our faculty members are experts in functional urology and have a lot of experience both with sacral neuromodulation and botulinum toxin and other therapies. So we're lucky we have a shiny Cashman from Adelaide. Australia. Dena Ultraman from Toronto, Mary and may petawatt. Vetter from not in France. I hope I pronounced that even partially right and rude. So hi from London.
+1
morning. Good afternoon. Good evening, wherever you're you are around the world. And Howard Goldman and I'm very happy to welcome you to this ICS state of the art presentation. Who, what, when and why? sacral neuromodulation or botulinum toxin for refractory overactive bladder. I'm from Cleveland, Ohio in the United States. And I serve as the chair of the ICS education committee. So we have a really excellent presentation set up we have an outstanding faculty. All of our faculty members are experts in functional urology and have a lot of experience both with sacral neuromodulation and botulinum toxin and other therapies. So we're lucky we have a shiny Cashman from Adelaide. Australia. Dena Ultraman from Toronto, Mary and may petawatt. Vetter from not in France. I hope I pronounced that even partially right and rude. So hi from London. Speaker 1
I also want to really thank Medtronic. Medtronic has sponsored this program and we wouldn't be able to put it together without the grant that they provided the ICS. So, we're all familiar with refractory overactive bladder patients who either fail conservative and medical management of overactive bladder, urgency, frequency, urge incontinence or could not tolerate the treatments and medications. And so it's not uncommon that we're faced with what's the next step. And I think if you look at refractory overactive bladder options there are a number of things that we do tibial nerve stimulation is popular, that can be done in different ways, either with surface patches with percutaneous electrodes, or there's now a lot of interest in various implantable technologies for tibial nerve stimulation. sacral neuromodulation has been around was approved in the United States in 1997. When I was finishing my fellowship, so I'm dating myself, but we've been doing that now for over 25 years, but the Lanham toxin was approved for overactive bladder uses probably about 15 Or maybe a little, maybe a few more years than that. So we've been using both of these for quite a while. If you look at some of  the national organizations This is the AQa SuFu. guideline for non neurogenic overactive bladder. Of course, we start with the history and physical your analysis, go on to behavioral treatments, pelvic floor, physiotherapy, pharmacologic management, but if they fail those things or can't tolerate them, then we go on to what in the US we call third line therapy, which is either botulinum toxin, of course, make sure you see the little note under here the patient has to be willing to perform intermittent catheterization if they have trouble or tibial nerve stimulation. Or sacral neuromodulation are all pretty much listed on a similar level. If you look at the E au guidelines, they recommend for these types of patients again, offer sacral nerve stimulation strong recommendation or botulinum toxin, also a strong recommendation. Of course, note that it's 100 units. Some of the studies done in the past have used higher doses, but the recommendation is 400 units and similar to the AOA caution they also mentioned that the physician should warn patients of the limited duration of responsibility on attacks and risk of UTI and the prolonged need the possible prolonged need for self catheterization. So despite that, I think both sacral neuromodulation and Baton have toxin, we would all agree are very highly effective treatments. If I think back to my residency just over 25 years ago, we didn't have any of these options. As a matter of fact, the only thing we had was oxybutynin and some other drugs that nobody uses for this reason right now. If I think just in my career, how far we've come and great options we have to treat people. It's really remarkable. But the question that faces us so you have the patient they have failed medication or they couldn't tolerate it. Perhaps they want to be on nerve stimulation. That's great. But if they've tried that and failed it or if they want to move on to either sacral neuromodulation, or botulinum toxin, how do you choose between them? Are there some patients who preferentially might benefit more from sacral neuromodulation whereas others might benefit more from botulinum toxin? How do we figure that out? And what do we do if somebody fails their first treatment? We just hang it up and say, okay, they're a failure, or do we perhaps go ahead and try the other treatment? So those are some of the questions that I'd like to try to answer, or at least discuss, and that's what our panelists will be discussing. So our agenda we're going to talk about are their patients who should preferentially get sick on their modulation work, perhaps some who should preferentially get it live toxic? What does the data show when you compare that? And either way, how do you move patients along this treatment pathway? So we're going to do this through the lectures of our panelists. We're also going to throughout this ask a few survey questions. It'd be interesting to see what our participants in our attendees think. So we'll see what everybody on the on the call thinks. And then at the end, we'll also have a panel discussion. The other important thing is I would really like to invite everybody as you're watching this to please feel free to enter questions into the chat. The panelists and myself, we will be on this. And so we'll be answering questions as they come up. So that'll make it very interesting. So please, please, please enter your questions into the chat during the lectures really anytime. We will seek to answer them right away as they come up.
the national organizations This is the AQa SuFu. guideline for non neurogenic overactive bladder. Of course, we start with the history and physical your analysis, go on to behavioral treatments, pelvic floor, physiotherapy, pharmacologic management, but if they fail those things or can't tolerate them, then we go on to what in the US we call third line therapy, which is either botulinum toxin, of course, make sure you see the little note under here the patient has to be willing to perform intermittent catheterization if they have trouble or tibial nerve stimulation. Or sacral neuromodulation are all pretty much listed on a similar level. If you look at the E au guidelines, they recommend for these types of patients again, offer sacral nerve stimulation strong recommendation or botulinum toxin, also a strong recommendation. Of course, note that it's 100 units. Some of the studies done in the past have used higher doses, but the recommendation is 400 units and similar to the AOA caution they also mentioned that the physician should warn patients of the limited duration of responsibility on attacks and risk of UTI and the prolonged need the possible prolonged need for self catheterization. So despite that, I think both sacral neuromodulation and Baton have toxin, we would all agree are very highly effective treatments. If I think back to my residency just over 25 years ago, we didn't have any of these options. As a matter of fact, the only thing we had was oxybutynin and some other drugs that nobody uses for this reason right now. If I think just in my career, how far we've come and great options we have to treat people. It's really remarkable. But the question that faces us so you have the patient they have failed medication or they couldn't tolerate it. Perhaps they want to be on nerve stimulation. That's great. But if they've tried that and failed it or if they want to move on to either sacral neuromodulation, or botulinum toxin, how do you choose between them? Are there some patients who preferentially might benefit more from sacral neuromodulation whereas others might benefit more from botulinum toxin? How do we figure that out? And what do we do if somebody fails their first treatment? We just hang it up and say, okay, they're a failure, or do we perhaps go ahead and try the other treatment? So those are some of the questions that I'd like to try to answer, or at least discuss, and that's what our panelists will be discussing. So our agenda we're going to talk about are their patients who should preferentially get sick on their modulation work, perhaps some who should preferentially get it live toxic? What does the data show when you compare that? And either way, how do you move patients along this treatment pathway? So we're going to do this through the lectures of our panelists. We're also going to throughout this ask a few survey questions. It'd be interesting to see what our participants in our attendees think. So we'll see what everybody on the on the call thinks. And then at the end, we'll also have a panel discussion. The other important thing is I would really like to invite everybody as you're watching this to please feel free to enter questions into the chat. The panelists and myself, we will be on this. And so we'll be answering questions as they come up. So that'll make it very interesting. So please, please, please enter your questions into the chat during the lectures really anytime. We will seek to answer them right away as they come up.
+1
the national organizations This is the AQa SuFu. guideline for non neurogenic overactive bladder. Of course, we start with the history and physical your analysis, go on to behavioral treatments, pelvic floor, physiotherapy, pharmacologic management, but if they fail those things or can't tolerate them, then we go on to what in the US we call third line therapy, which is either botulinum toxin, of course, make sure you see the little note under here the patient has to be willing to perform intermittent catheterization if they have trouble or tibial nerve stimulation. Or sacral neuromodulation are all pretty much listed on a similar level. If you look at the E au guidelines, they recommend for these types of patients again, offer sacral nerve stimulation strong recommendation or botulinum toxin, also a strong recommendation. Of course, note that it's 100 units. Some of the studies done in the past have used higher doses, but the recommendation is 400 units and similar to the AOA caution they also mentioned that the physician should warn patients of the limited duration of responsibility on attacks and risk of UTI and the prolonged need the possible prolonged need for self catheterization. So despite that, I think both sacral neuromodulation and Baton have toxin, we would all agree are very highly effective treatments. If I think back to my residency just over 25 years ago, we didn't have any of these options. As a matter of fact, the only thing we had was oxybutynin and some other drugs that nobody uses for this reason right now. If I think just in my career, how far we've come and great options we have to treat people. It's really remarkable. But the question that faces us so you have the patient they have failed medication or they couldn't tolerate it. Perhaps they want to be on nerve stimulation. That's great. But if they've tried that and failed it or if they want to move on to either sacral neuromodulation, or botulinum toxin, how do you choose between them? Are there some patients who preferentially might benefit more from sacral neuromodulation whereas others might benefit more from botulinum toxin? How do we figure that out? And what do we do if somebody fails their first treatment? We just hang it up and say, okay, they're a failure, or do we perhaps go ahead and try the other treatment? So those are some of the questions that I'd like to try to answer, or at least discuss, and that's what our panelists will be discussing. So our agenda we're going to talk about are their patients who should preferentially get sick on their modulation work, perhaps some who should preferentially get it live toxic? What does the data show when you compare that? And either way, how do you move patients along this treatment pathway? So we're going to do this through the lectures of our panelists. We're also going to throughout this ask a few survey questions. It'd be interesting to see what our participants in our attendees think. So we'll see what everybody on the on the call thinks. And then at the end, we'll also have a panel discussion. The other important thing is I would really like to invite everybody as you're watching this to please feel free to enter questions into the chat. The panelists and myself, we will be on this. And so we'll be answering questions as they come up. So that'll make it very interesting. So please, please, please enter your questions into the chat during the lectures really anytime. We will seek to answer them right away as they come up. Speaker 2
Okay, thank you, Howard. My name is Roger from the ICS office and welcome to the masterclass I just like to read out the first of our poll question is here. So he's one, a 64 year old woman has bothersome new UI and has failed conservative therapies and two medications. She also has some fecal incontinence, which treatment would you choose for her and to the your answers on the older now?
Speaker 2
Thank you, right I'm seeing the answers coming in. Wonderful. Okay. Let's reveal the results there. So we have 6% saying a botulinum toxin and 94% B sacral. neuromodulation. Okay. Thanks very much, everybody. I'm sure how it will be discussing these results with you shortly. And then there's the results you can see and we will move on to the next presentation.
Speaker 3
Hi, 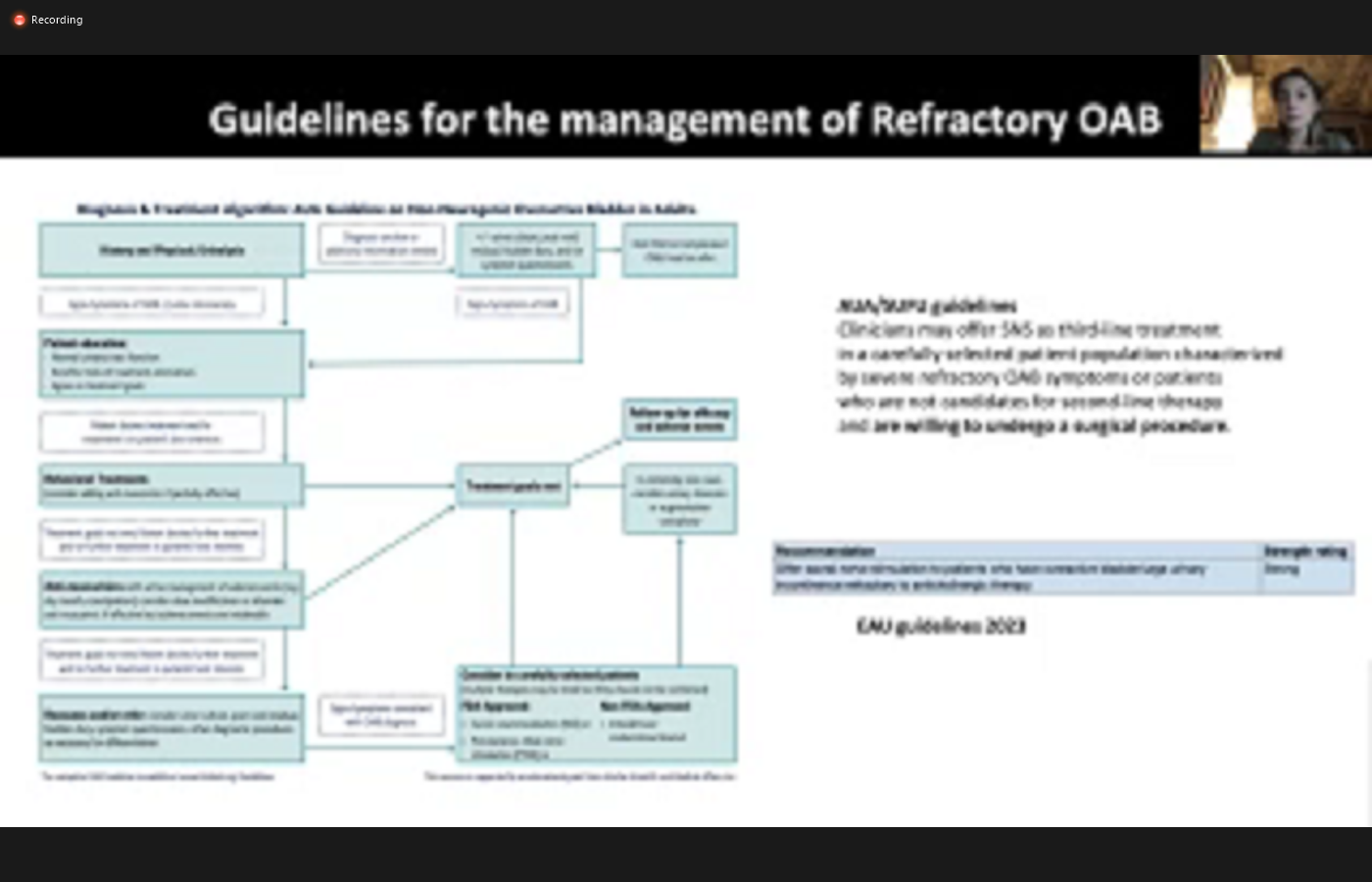
 everyone, I'm Marie me bear with them. You will adjust from friends walking, not University Hospital, in functional neurology and neuro Urology. So it's my pleasure to discuss with you today which patient with a refractory way b should get SNM preferentially. So first of all, as you all know, s&s is FDA approved in the treatment of gravy. It's recommended as a third line of treatment in a way as usual. And in the Recently Updated EU guidelines in some selected patients with refractory will be seen terms who are willing to undergo a surgical procedure. The long term results of SLM in wavy have been reported by several prospective studies. It's important to note that most studies reporting on long term data refer to older as an end technology and outcomes may therefore be improved, especially in terms of complications with the newer technologies in carefully selected patients, as an as is an appropriate therapy with durable treatment effects. Indeed, in the insights study, the success rate was still high at 2% at five year postimplantation. Regarding the adverse events the insights study on will be patient, published in 2080 18 showed the most common adverse events reported that
everyone, I'm Marie me bear with them. You will adjust from friends walking, not University Hospital, in functional neurology and neuro Urology. So it's my pleasure to discuss with you today which patient with a refractory way b should get SNM preferentially. So first of all, as you all know, s&s is FDA approved in the treatment of gravy. It's recommended as a third line of treatment in a way as usual. And in the Recently Updated EU guidelines in some selected patients with refractory will be seen terms who are willing to undergo a surgical procedure. The long term results of SLM in wavy have been reported by several prospective studies. It's important to note that most studies reporting on long term data refer to older as an end technology and outcomes may therefore be improved, especially in terms of complications with the newer technologies in carefully selected patients, as an as is an appropriate therapy with durable treatment effects. Indeed, in the insights study, the success rate was still high at 2% at five year postimplantation. Regarding the adverse events the insights study on will be patient, published in 2080 18 showed the most common adverse events reported that  five years were also an undesirable change in stimulation, and implant side pain. In 50% of cases. However, thanks to smaller new devices, it's possible that the rate of pain will decrease in the future. reoperation rate was reported at five year in the insights study 31% of reparation were due to an adverse event and 33.5 were for battery replacement. Permanent exchange rate was 90% with apron five, related to lack or loss of efficacy. Both Botox and snsf effective therapies for refractory OB But they are not equivalent. As an M is a restorative therapy and returns function back to the patient. Botox takes away bladder function and may impact voiding efficiency, where whereas SNS can treat it. Finally buttocks as a local effect, whereas SNS is more holistic and can also improve other concomitant pelvic floor dysfunction. Consideration of other pelvic floor dysfunction is essential in order to tailor treatment to individual patients characteristics. Indeed, it's now known that some comorbidities may affect a baby. And it's also known then that SNS can improve some vulnerabilities and appears to be the best option for some specific way b phenotypes. As an M is an effective treatment for
five years were also an undesirable change in stimulation, and implant side pain. In 50% of cases. However, thanks to smaller new devices, it's possible that the rate of pain will decrease in the future. reoperation rate was reported at five year in the insights study 31% of reparation were due to an adverse event and 33.5 were for battery replacement. Permanent exchange rate was 90% with apron five, related to lack or loss of efficacy. Both Botox and snsf effective therapies for refractory OB But they are not equivalent. As an M is a restorative therapy and returns function back to the patient. Botox takes away bladder function and may impact voiding efficiency, where whereas SNS can treat it. Finally buttocks as a local effect, whereas SNS is more holistic and can also improve other concomitant pelvic floor dysfunction. Consideration of other pelvic floor dysfunction is essential in order to tailor treatment to individual patients characteristics. Indeed, it's now known that some comorbidities may affect a baby. And it's also known then that SNS can improve some vulnerabilities and appears to be the best option for some specific way b phenotypes. As an M is an effective treatment for  for syndrome and non obstructive urinary retention. In 2007, funkier Brook progressed five year follow up results of a prospective worldwide clinical study on SNM in non obstructive urinary retention with a success rate of 71% with an average number of catheterizations per day decreased from five a baseline to two at five years after implantation. In some selected patients, SNS may be the preferred option in particular in case of MCs, let's only be avoiding this function. And I'm so impatient at risk of retention with Botox especially with a bow contractor that was an inpatient not able to serve catheterized regarding related to cognitive impairment, or for example, a blue line disability. SNS is a FDA approved treatment option in fecal incontinence. Conservative medical measures are the first line treatment for fecal incontinence. However, SNM should be considered as the second line of treatment in most patient with fecal incontinence, physicians should consider SNM if the patient has failed medical measures, as as an MS been shown to be superior to best medical treatment. Results of pool pooled analyzes as suggested that 79% of patients with permanent imprint for chronic stimulation experience at least 50% improvement in in continuous episodes in the short term, while 84% achieved this endpoint, with three years of follow up. Published series in children and adult patients with OB and fecal incontinence reported improvement in bus theme terms after s&m implant and in the ICS best practice statement for use of sacral neuromodulation published in 2017. The authors recommend SNS in these patients who is combined renourish inborn symptoms. There is limited evidence supporting the role of SMM or patient with interstitial cystitis bladder pain syndrome. However, s&m may be an option in these patients, not responding to conservative therapies after appropriate assessment and multidisciplinary team review. The AQa ICBS guidelines list as an as a fourth line therapy. In some selected patients with mixed let's for example, refractory way b and chronic pelvic pain, SNS may be the preferred option compared to Botox, as it may play a role in pain and also may not affect on voiding efficiency. Indeed, intermittent self catheterization may be difficult to perform in these patients. Similarly, patients who suffer from both voiding dysfunction and chronic pelvic pain may benefit from SNS as can improve both symptoms. New rechargeable devices with longer battery life could be of particular interest to these patients, whereas stimulation can sometimes be of a amplitude. There is also limited evidence on the role of SNM in patients with neuronal if you're a winner retract this function. Array recently published systematic review by a woman from 2021 based on 47. Studies with mixed neurological disease and mixed last reported a success rate of success rate of 60% during the test phase, and inpatient with definitive implant. The rate of efficacy was still high at 84%. However, SNS cannot be offered in all neurogenic patient indeed, SMS is not an option for patients at high risk of upper arena retract deterioration, especially for patients with complete spinal cord injury with it was also active dyskinesia where intermittent self catheterization was encoded with overtraining toxin injection is the standard of care. Inpatient, we're able to perform self catheterization Of course, and thanks to the new devices for SNS that are full body MRI compatible, there are no longer a contraindication for patients with newly neurological disease, who require an MRI of the pelvis or of the spine so in summary, SNS may be the preferred option in patients with mixed symptoms depending on the patient's characteristics. And it may also be suggested in some selective neurogenic patient at low risk of arena retracted valuation. The patient's preference and lifestyle are also crucial for customizing treatment in the shared decision making process. Thank you.
for syndrome and non obstructive urinary retention. In 2007, funkier Brook progressed five year follow up results of a prospective worldwide clinical study on SNM in non obstructive urinary retention with a success rate of 71% with an average number of catheterizations per day decreased from five a baseline to two at five years after implantation. In some selected patients, SNS may be the preferred option in particular in case of MCs, let's only be avoiding this function. And I'm so impatient at risk of retention with Botox especially with a bow contractor that was an inpatient not able to serve catheterized regarding related to cognitive impairment, or for example, a blue line disability. SNS is a FDA approved treatment option in fecal incontinence. Conservative medical measures are the first line treatment for fecal incontinence. However, SNM should be considered as the second line of treatment in most patient with fecal incontinence, physicians should consider SNM if the patient has failed medical measures, as as an MS been shown to be superior to best medical treatment. Results of pool pooled analyzes as suggested that 79% of patients with permanent imprint for chronic stimulation experience at least 50% improvement in in continuous episodes in the short term, while 84% achieved this endpoint, with three years of follow up. Published series in children and adult patients with OB and fecal incontinence reported improvement in bus theme terms after s&m implant and in the ICS best practice statement for use of sacral neuromodulation published in 2017. The authors recommend SNS in these patients who is combined renourish inborn symptoms. There is limited evidence supporting the role of SMM or patient with interstitial cystitis bladder pain syndrome. However, s&m may be an option in these patients, not responding to conservative therapies after appropriate assessment and multidisciplinary team review. The AQa ICBS guidelines list as an as a fourth line therapy. In some selected patients with mixed let's for example, refractory way b and chronic pelvic pain, SNS may be the preferred option compared to Botox, as it may play a role in pain and also may not affect on voiding efficiency. Indeed, intermittent self catheterization may be difficult to perform in these patients. Similarly, patients who suffer from both voiding dysfunction and chronic pelvic pain may benefit from SNS as can improve both symptoms. New rechargeable devices with longer battery life could be of particular interest to these patients, whereas stimulation can sometimes be of a amplitude. There is also limited evidence on the role of SNM in patients with neuronal if you're a winner retract this function. Array recently published systematic review by a woman from 2021 based on 47. Studies with mixed neurological disease and mixed last reported a success rate of success rate of 60% during the test phase, and inpatient with definitive implant. The rate of efficacy was still high at 84%. However, SNS cannot be offered in all neurogenic patient indeed, SMS is not an option for patients at high risk of upper arena retract deterioration, especially for patients with complete spinal cord injury with it was also active dyskinesia where intermittent self catheterization was encoded with overtraining toxin injection is the standard of care. Inpatient, we're able to perform self catheterization Of course, and thanks to the new devices for SNS that are full body MRI compatible, there are no longer a contraindication for patients with newly neurological disease, who require an MRI of the pelvis or of the spine so in summary, SNS may be the preferred option in patients with mixed symptoms depending on the patient's characteristics. And it may also be suggested in some selective neurogenic patient at low risk of arena retracted valuation. The patient's preference and lifestyle are also crucial for customizing treatment in the shared decision making process. Thank you.
+2
everyone, I'm Marie me bear with them. You will adjust from friends walking, not University Hospital, in functional neurology and neuro Urology. So it's my pleasure to discuss with you today which patient with a refractory way b should get SNM preferentially. So first of all, as you all know, s&s is FDA approved in the treatment of gravy. It's recommended as a third line of treatment in a way as usual. And in the Recently Updated EU guidelines in some selected patients with refractory will be seen terms who are willing to undergo a surgical procedure. The long term results of SLM in wavy have been reported by several prospective studies. It's important to note that most studies reporting on long term data refer to older as an end technology and outcomes may therefore be improved, especially in terms of complications with the newer technologies in carefully selected patients, as an as is an appropriate therapy with durable treatment effects. Indeed, in the insights study, the success rate was still high at 2% at five year postimplantation. Regarding the adverse events the insights study on will be patient, published in 2080 18 showed the most common adverse events reported that +1
five years were also an undesirable change in stimulation, and implant side pain. In 50% of cases. However, thanks to smaller new devices, it's possible that the rate of pain will decrease in the future. reoperation rate was reported at five year in the insights study 31% of reparation were due to an adverse event and 33.5 were for battery replacement. Permanent exchange rate was 90% with apron five, related to lack or loss of efficacy. Both Botox and snsf effective therapies for refractory OB But they are not equivalent. As an M is a restorative therapy and returns function back to the patient. Botox takes away bladder function and may impact voiding efficiency, where whereas SNS can treat it. Finally buttocks as a local effect, whereas SNS is more holistic and can also improve other concomitant pelvic floor dysfunction. Consideration of other pelvic floor dysfunction is essential in order to tailor treatment to individual patients characteristics. Indeed, it's now known that some comorbidities may affect a baby. And it's also known then that SNS can improve some vulnerabilities and appears to be the best option for some specific way b phenotypes. As an M is an effective treatment for +1
for syndrome and non obstructive urinary retention. In 2007, funkier Brook progressed five year follow up results of a prospective worldwide clinical study on SNM in non obstructive urinary retention with a success rate of 71% with an average number of catheterizations per day decreased from five a baseline to two at five years after implantation. In some selected patients, SNS may be the preferred option in particular in case of MCs, let's only be avoiding this function. And I'm so impatient at risk of retention with Botox especially with a bow contractor that was an inpatient not able to serve catheterized regarding related to cognitive impairment, or for example, a blue line disability. SNS is a FDA approved treatment option in fecal incontinence. Conservative medical measures are the first line treatment for fecal incontinence. However, SNM should be considered as the second line of treatment in most patient with fecal incontinence, physicians should consider SNM if the patient has failed medical measures, as as an MS been shown to be superior to best medical treatment. Results of pool pooled analyzes as suggested that 79% of patients with permanent imprint for chronic stimulation experience at least 50% improvement in in continuous episodes in the short term, while 84% achieved this endpoint, with three years of follow up. Published series in children and adult patients with OB and fecal incontinence reported improvement in bus theme terms after s&m implant and in the ICS best practice statement for use of sacral neuromodulation published in 2017. The authors recommend SNS in these patients who is combined renourish inborn symptoms. There is limited evidence supporting the role of SMM or patient with interstitial cystitis bladder pain syndrome. However, s&m may be an option in these patients, not responding to conservative therapies after appropriate assessment and multidisciplinary team review. The AQa ICBS guidelines list as an as a fourth line therapy. In some selected patients with mixed let's for example, refractory way b and chronic pelvic pain, SNS may be the preferred option compared to Botox, as it may play a role in pain and also may not affect on voiding efficiency. Indeed, intermittent self catheterization may be difficult to perform in these patients. Similarly, patients who suffer from both voiding dysfunction and chronic pelvic pain may benefit from SNS as can improve both symptoms. New rechargeable devices with longer battery life could be of particular interest to these patients, whereas stimulation can sometimes be of a amplitude. There is also limited evidence on the role of SNM in patients with neuronal if you're a winner retract this function. Array recently published systematic review by a woman from 2021 based on 47. Studies with mixed neurological disease and mixed last reported a success rate of success rate of 60% during the test phase, and inpatient with definitive implant. The rate of efficacy was still high at 84%. However, SNS cannot be offered in all neurogenic patient indeed, SMS is not an option for patients at high risk of upper arena retract deterioration, especially for patients with complete spinal cord injury with it was also active dyskinesia where intermittent self catheterization was encoded with overtraining toxin injection is the standard of care. Inpatient, we're able to perform self catheterization Of course, and thanks to the new devices for SNS that are full body MRI compatible, there are no longer a contraindication for patients with newly neurological disease, who require an MRI of the pelvis or of the spine so in summary, SNS may be the preferred option in patients with mixed symptoms depending on the patient's characteristics. And it may also be suggested in some selective neurogenic patient at low risk of arena retracted valuation. The patient's preference and lifestyle are also crucial for customizing treatment in the shared decision making process. Thank you. Speaker 2
Okay, so moving on. To our second case question here. We have a 53 year old woman with significant urinary frequency and urgency has failed conservative therapies and medication. She has no bowel issues. Post post void residual is 10 milliliters and she has never had a UTI. Which treatment would you choose for her? A botulinum toxin or B sacral. Neuro modulation I see your answers now. Please
Unknown Speaker
all right. I see lots coming in.
Speaker 2
Okay, last few moments to answer this poll. Let's hear which treatments you would choose for this case?
Speaker 2
Okay, all right. So the answers are in let's have a look at the results here. So we have 70% of you would choose a botulinum toxin with 30% thing sacral neuromodulation. And feel free to jump in the chat. Let us know why. You would make those choices. All right. Thanks very much. Let's move on to the next presentation.
Speaker 4
Thank  you for my introduction, Howard. And it's my pleasure to speak about Basilar tomb toxin as an option for refractory overactive bladder. Here in our master class today. My disclosures as you can see, I think when we start talking about any topic, it's quite key for us to ensure that we start with the definition of what refractory overactive bladder might be. The ICS definition of an overactive bladder is as you can see there increased urgency usually accompanied by increasing daytime frequency and or nocturia with urinary incontinence, with or without urinary incontinence. In the absence of infection or detectable disease. Now in our situation, we'll be looking at refractory overactive bladder, where I believe what we're really looking at is a failure of first line therapy, or indeed poor response to first line therapy. In my case, I'm defining first line therapy as a combination of behavioral management options, including bladder retraining, pelvic floor exercises, but also of course medications. We do have a significant proportion of patients that don't tolerate their medications are on medications for overactive bladder. And I actually put these people in the refractory overactive bladder community as well. The quoted rates in
you for my introduction, Howard. And it's my pleasure to speak about Basilar tomb toxin as an option for refractory overactive bladder. Here in our master class today. My disclosures as you can see, I think when we start talking about any topic, it's quite key for us to ensure that we start with the definition of what refractory overactive bladder might be. The ICS definition of an overactive bladder is as you can see there increased urgency usually accompanied by increasing daytime frequency and or nocturia with urinary incontinence, with or without urinary incontinence. In the absence of infection or detectable disease. Now in our situation, we'll be looking at refractory overactive bladder, where I believe what we're really looking at is a failure of first line therapy, or indeed poor response to first line therapy. In my case, I'm defining first line therapy as a combination of behavioral management options, including bladder retraining, pelvic floor exercises, but also of course medications. We do have a significant proportion of patients that don't tolerate their medications are on medications for overactive bladder. And I actually put these people in the refractory overactive bladder community as well. The quoted rates in  the literature are between 30 to 50%. So realistically, what we're looking at is half of our patients presenting with primary overactive bladder will now fall into this secondary refractory group. I think that when you're talking about third line therapies, the key here is a combined decision making approach. And I think part of that decision making requires us discussing the efficacy of the therapy involved, how easy it is to access that therapy for a patient from a different geographical area. Of course their medical history will have a part to play in that and the ability to undertake long term monitoring. Now in certain health systems, financial considerations are important. Certainly speaking in Australia, you would want to be thinking about whether or not this is in the private sector, the ability to manage a device, so comparability and of course, ultimately patient preference based on all of the things that we've talked about. So realistically, when we're talking about botulinum toxin is a primary therapy for a patient with refractory overactive bladder. Are we talking about the perfect patient for Botox? Or are we talking about a patient who cannot manage sacral neuromodulation which is our alternative therapy for refractory overactive bladder? Is it that simple. In medicine I find nothing ever is. So how do I look at this group of patients? How do I think actually botulinum toxin might be a better option for you? I think that technical considerations are really important. I mean, do you have a sacrum? Is your sacrum complete or anatomically normal? Is your body mass index going to make access into that third sacral frame and easy? Do we have access to radiology to allow radiologic guidance for the insertion of your basic evaluation? Do we have a needle that's long enough to access the anterior margin of that sacral plate? Then of course we consider our patient factors. If we're considering neuromodulation Do you have excellent hand function? Do you have excellent cognition and you're able then to manage your handpiece or your hand device for your ongoing monitoring? But if you're thinking botulinum toxin and you are that 5% of patients who are unable to avoid in that first six to eight week period, are you able to manage an integrated catheter overhaul to insert it? Either actually put disease factors here separately, but I think of course, it's tied into our technical and patient factors. If you have a progressive deteriorating disease, where cognition or mobility or hand function will be impaired. I think that's an important consideration in considering how you would then progress with your patient bladder. Finally, when you pull all of that together, if we go back to that original slide I demonstrated you should be able to do a decision or make a decision on therapy that's patient centered, but also thinking ahead so that this is an effective therapy for the patient in the long term. So in incorporating all of these factors in your decision making, I think that this table summarizes what we've talked about, but also summarizes how we might decide one patient might be better for therapy versus the other. So for me, I will be looking at a patient who has difficult anatomy, anatomy or unsuitable anatomy. For example, a spinal bifida patient with an incompletely formed sacral sacral, or even previous significant sacral fractures, rendering that s3 nerve root difficult to access. Now that might require an MRI to ascertain. In Australia, when we are undertaking that first stage for neuromodulation, or basic evaluation, the patient does undergo sedation. I know this may not be the same across the geographies that we have on our panel today. So suitability for sedation also falls into an important consideration for us in the southern hemisphere. Do they have other pain modulation devices? How many sides of that upper outer quadrant of the buttock are they utilizing for their batteries? And of course, the difficult consideration about age now I think this is adjustable. And in the modern day, an older patient is not a definite or absolute contraindication for neuromodulation but could certainly be a consideration in the long term. So I seem to be falling back into saying, hey, if we are picking botulinum toxin is therapy for refractory overactive bladder. We're actually looking at patients who might be unsuitable for neuromodulation then there are two sides of a single coin. Now if I flip that, and I say okay, we're talking about botulinum toxin as a primary therapy for refractory overactive bladder, you have excellent hand function, the ability and the opportunity to undertake intermittent catheterization if required, or certainly in some cases already. undertaking it for dysfunctional voiding. Excellent cognition in mobility, perhaps already undertaking urine containment in the form of a suprapubic catheter. With long term disease progression, where we're thinking, mobility is going to be an issue. function is going to be issue social support. And engagement is going to be an issue. Then I think I will be prioritizing botulinum toxin to manage the truth of reactivity. So you're a dynamically proven overactive bladder refractory to oral therapy as my primary treatment option in that population that latterly then feeds into your dynamic parameters and perhaps disease factors, because overactive bladder ease heterogenous multiple factors will input into the severity, the fluctuation and progression of the disease. And I think based on bladder capacity also has a part to play someone with a functional capacity that's very low. I'll be considering for botulinum toxin over neuromodulation because in my opinion, and based on the evidence there is a higher likelihood of increasing that bladder capacity, admittedly on average, but only 100 mils compliance is an interesting one. Does poor compliance denote poor response to botulinum toxin? Possibly. But does poor compliance then imply the poor response to neuromodulation? Possibly so I think that is a soft consideration. There is very little if any evidence to support the use of neuromodulation in hostile depressions, particularly in our neurogenic population. And I think if that is present, we really should be looking at objective evidence that is suitable to make a clinical decision that's helpful in the long term management of that bladder and that patient. And in those cases, I strongly believe botulinum toxin might overtake neuromodulation as an appropriate therapeutic option. Now in patients already just demonstrating dysfunctional voiding. This may indeed make it more likely to require integrated catheterization following botulinum toxin injection, and this population might be better served undertaking neuromodulation ultimately, this is a combined decision making approach. Our key goal is to ensure that the patient is safe, happy and their long term health goals are achieved. How do we do that? By clear, concise and thoughtful decision making, discussing what clear treatment options are, what their goals are and how they match with the treatment options. What works with their lifestyle, what helps them get to school, get to work, get to engage in society better, and what supports exist, ultimately, what do they want? And how can we achieve that within the constraints
the literature are between 30 to 50%. So realistically, what we're looking at is half of our patients presenting with primary overactive bladder will now fall into this secondary refractory group. I think that when you're talking about third line therapies, the key here is a combined decision making approach. And I think part of that decision making requires us discussing the efficacy of the therapy involved, how easy it is to access that therapy for a patient from a different geographical area. Of course their medical history will have a part to play in that and the ability to undertake long term monitoring. Now in certain health systems, financial considerations are important. Certainly speaking in Australia, you would want to be thinking about whether or not this is in the private sector, the ability to manage a device, so comparability and of course, ultimately patient preference based on all of the things that we've talked about. So realistically, when we're talking about botulinum toxin is a primary therapy for a patient with refractory overactive bladder. Are we talking about the perfect patient for Botox? Or are we talking about a patient who cannot manage sacral neuromodulation which is our alternative therapy for refractory overactive bladder? Is it that simple. In medicine I find nothing ever is. So how do I look at this group of patients? How do I think actually botulinum toxin might be a better option for you? I think that technical considerations are really important. I mean, do you have a sacrum? Is your sacrum complete or anatomically normal? Is your body mass index going to make access into that third sacral frame and easy? Do we have access to radiology to allow radiologic guidance for the insertion of your basic evaluation? Do we have a needle that's long enough to access the anterior margin of that sacral plate? Then of course we consider our patient factors. If we're considering neuromodulation Do you have excellent hand function? Do you have excellent cognition and you're able then to manage your handpiece or your hand device for your ongoing monitoring? But if you're thinking botulinum toxin and you are that 5% of patients who are unable to avoid in that first six to eight week period, are you able to manage an integrated catheter overhaul to insert it? Either actually put disease factors here separately, but I think of course, it's tied into our technical and patient factors. If you have a progressive deteriorating disease, where cognition or mobility or hand function will be impaired. I think that's an important consideration in considering how you would then progress with your patient bladder. Finally, when you pull all of that together, if we go back to that original slide I demonstrated you should be able to do a decision or make a decision on therapy that's patient centered, but also thinking ahead so that this is an effective therapy for the patient in the long term. So in incorporating all of these factors in your decision making, I think that this table summarizes what we've talked about, but also summarizes how we might decide one patient might be better for therapy versus the other. So for me, I will be looking at a patient who has difficult anatomy, anatomy or unsuitable anatomy. For example, a spinal bifida patient with an incompletely formed sacral sacral, or even previous significant sacral fractures, rendering that s3 nerve root difficult to access. Now that might require an MRI to ascertain. In Australia, when we are undertaking that first stage for neuromodulation, or basic evaluation, the patient does undergo sedation. I know this may not be the same across the geographies that we have on our panel today. So suitability for sedation also falls into an important consideration for us in the southern hemisphere. Do they have other pain modulation devices? How many sides of that upper outer quadrant of the buttock are they utilizing for their batteries? And of course, the difficult consideration about age now I think this is adjustable. And in the modern day, an older patient is not a definite or absolute contraindication for neuromodulation but could certainly be a consideration in the long term. So I seem to be falling back into saying, hey, if we are picking botulinum toxin is therapy for refractory overactive bladder. We're actually looking at patients who might be unsuitable for neuromodulation then there are two sides of a single coin. Now if I flip that, and I say okay, we're talking about botulinum toxin as a primary therapy for refractory overactive bladder, you have excellent hand function, the ability and the opportunity to undertake intermittent catheterization if required, or certainly in some cases already. undertaking it for dysfunctional voiding. Excellent cognition in mobility, perhaps already undertaking urine containment in the form of a suprapubic catheter. With long term disease progression, where we're thinking, mobility is going to be an issue. function is going to be issue social support. And engagement is going to be an issue. Then I think I will be prioritizing botulinum toxin to manage the truth of reactivity. So you're a dynamically proven overactive bladder refractory to oral therapy as my primary treatment option in that population that latterly then feeds into your dynamic parameters and perhaps disease factors, because overactive bladder ease heterogenous multiple factors will input into the severity, the fluctuation and progression of the disease. And I think based on bladder capacity also has a part to play someone with a functional capacity that's very low. I'll be considering for botulinum toxin over neuromodulation because in my opinion, and based on the evidence there is a higher likelihood of increasing that bladder capacity, admittedly on average, but only 100 mils compliance is an interesting one. Does poor compliance denote poor response to botulinum toxin? Possibly. But does poor compliance then imply the poor response to neuromodulation? Possibly so I think that is a soft consideration. There is very little if any evidence to support the use of neuromodulation in hostile depressions, particularly in our neurogenic population. And I think if that is present, we really should be looking at objective evidence that is suitable to make a clinical decision that's helpful in the long term management of that bladder and that patient. And in those cases, I strongly believe botulinum toxin might overtake neuromodulation as an appropriate therapeutic option. Now in patients already just demonstrating dysfunctional voiding. This may indeed make it more likely to require integrated catheterization following botulinum toxin injection, and this population might be better served undertaking neuromodulation ultimately, this is a combined decision making approach. Our key goal is to ensure that the patient is safe, happy and their long term health goals are achieved. How do we do that? By clear, concise and thoughtful decision making, discussing what clear treatment options are, what their goals are and how they match with the treatment options. What works with their lifestyle, what helps them get to school, get to work, get to engage in society better, and what supports exist, ultimately, what do they want? And how can we achieve that within the constraints 
 of the therapies available to us.
of the therapies available to us.
+1
you for my introduction, Howard. And it's my pleasure to speak about Basilar tomb toxin as an option for refractory overactive bladder. Here in our master class today. My disclosures as you can see, I think when we start talking about any topic, it's quite key for us to ensure that we start with the definition of what refractory overactive bladder might be. The ICS definition of an overactive bladder is as you can see there increased urgency usually accompanied by increasing daytime frequency and or nocturia with urinary incontinence, with or without urinary incontinence. In the absence of infection or detectable disease. Now in our situation, we'll be looking at refractory overactive bladder, where I believe what we're really looking at is a failure of first line therapy, or indeed poor response to first line therapy. In my case, I'm defining first line therapy as a combination of behavioral management options, including bladder retraining, pelvic floor exercises, but also of course medications. We do have a significant proportion of patients that don't tolerate their medications are on medications for overactive bladder. And I actually put these people in the refractory overactive bladder community as well. The quoted rates in +1
the literature are between 30 to 50%. So realistically, what we're looking at is half of our patients presenting with primary overactive bladder will now fall into this secondary refractory group. I think that when you're talking about third line therapies, the key here is a combined decision making approach. And I think part of that decision making requires us discussing the efficacy of the therapy involved, how easy it is to access that therapy for a patient from a different geographical area. Of course their medical history will have a part to play in that and the ability to undertake long term monitoring. Now in certain health systems, financial considerations are important. Certainly speaking in Australia, you would want to be thinking about whether or not this is in the private sector, the ability to manage a device, so comparability and of course, ultimately patient preference based on all of the things that we've talked about. So realistically, when we're talking about botulinum toxin is a primary therapy for a patient with refractory overactive bladder. Are we talking about the perfect patient for Botox? Or are we talking about a patient who cannot manage sacral neuromodulation which is our alternative therapy for refractory overactive bladder? Is it that simple. In medicine I find nothing ever is. So how do I look at this group of patients? How do I think actually botulinum toxin might be a better option for you? I think that technical considerations are really important. I mean, do you have a sacrum? Is your sacrum complete or anatomically normal? Is your body mass index going to make access into that third sacral frame and easy? Do we have access to radiology to allow radiologic guidance for the insertion of your basic evaluation? Do we have a needle that's long enough to access the anterior margin of that sacral plate? Then of course we consider our patient factors. If we're considering neuromodulation Do you have excellent hand function? Do you have excellent cognition and you're able then to manage your handpiece or your hand device for your ongoing monitoring? But if you're thinking botulinum toxin and you are that 5% of patients who are unable to avoid in that first six to eight week period, are you able to manage an integrated catheter overhaul to insert it? Either actually put disease factors here separately, but I think of course, it's tied into our technical and patient factors. If you have a progressive deteriorating disease, where cognition or mobility or hand function will be impaired. I think that's an important consideration in considering how you would then progress with your patient bladder. Finally, when you pull all of that together, if we go back to that original slide I demonstrated you should be able to do a decision or make a decision on therapy that's patient centered, but also thinking ahead so that this is an effective therapy for the patient in the long term. So in incorporating all of these factors in your decision making, I think that this table summarizes what we've talked about, but also summarizes how we might decide one patient might be better for therapy versus the other. So for me, I will be looking at a patient who has difficult anatomy, anatomy or unsuitable anatomy. For example, a spinal bifida patient with an incompletely formed sacral sacral, or even previous significant sacral fractures, rendering that s3 nerve root difficult to access. Now that might require an MRI to ascertain. In Australia, when we are undertaking that first stage for neuromodulation, or basic evaluation, the patient does undergo sedation. I know this may not be the same across the geographies that we have on our panel today. So suitability for sedation also falls into an important consideration for us in the southern hemisphere. Do they have other pain modulation devices? How many sides of that upper outer quadrant of the buttock are they utilizing for their batteries? And of course, the difficult consideration about age now I think this is adjustable. And in the modern day, an older patient is not a definite or absolute contraindication for neuromodulation but could certainly be a consideration in the long term. So I seem to be falling back into saying, hey, if we are picking botulinum toxin is therapy for refractory overactive bladder. We're actually looking at patients who might be unsuitable for neuromodulation then there are two sides of a single coin. Now if I flip that, and I say okay, we're talking about botulinum toxin as a primary therapy for refractory overactive bladder, you have excellent hand function, the ability and the opportunity to undertake intermittent catheterization if required, or certainly in some cases already. undertaking it for dysfunctional voiding. Excellent cognition in mobility, perhaps already undertaking urine containment in the form of a suprapubic catheter. With long term disease progression, where we're thinking, mobility is going to be an issue. function is going to be issue social support. And engagement is going to be an issue. Then I think I will be prioritizing botulinum toxin to manage the truth of reactivity. So you're a dynamically proven overactive bladder refractory to oral therapy as my primary treatment option in that population that latterly then feeds into your dynamic parameters and perhaps disease factors, because overactive bladder ease heterogenous multiple factors will input into the severity, the fluctuation and progression of the disease. And I think based on bladder capacity also has a part to play someone with a functional capacity that's very low. I'll be considering for botulinum toxin over neuromodulation because in my opinion, and based on the evidence there is a higher likelihood of increasing that bladder capacity, admittedly on average, but only 100 mils compliance is an interesting one. Does poor compliance denote poor response to botulinum toxin? Possibly. But does poor compliance then imply the poor response to neuromodulation? Possibly so I think that is a soft consideration. There is very little if any evidence to support the use of neuromodulation in hostile depressions, particularly in our neurogenic population. And I think if that is present, we really should be looking at objective evidence that is suitable to make a clinical decision that's helpful in the long term management of that bladder and that patient. And in those cases, I strongly believe botulinum toxin might overtake neuromodulation as an appropriate therapeutic option. Now in patients already just demonstrating dysfunctional voiding. This may indeed make it more likely to require integrated catheterization following botulinum toxin injection, and this population might be better served undertaking neuromodulation ultimately, this is a combined decision making approach. Our key goal is to ensure that the patient is safe, happy and their long term health goals are achieved. How do we do that? By clear, concise and thoughtful decision making, discussing what clear treatment options are, what their goals are and how they match with the treatment options. What works with their lifestyle, what helps them get to school, get to work, get to engage in society better, and what supports exist, ultimately, what do they want? And how can we achieve that within the constraints +7
of the therapies available to us.